Unit 2: Core Interventions (The Protocol)¶
Chapter 2.8: Metabolic Health & Nutrition Timing¶
[CHONK: 1-minute summary]
What you'll learn in this chapter:
- What metabolic health actually means and why it matters for longevity
- Metabolic flexibility: your body's ability to switch between fuel sources (and why it declines with age)
- Practical blood sugar management strategies coaches can implement
- Time-restricted eating: evidence, protocols, and appropriate caveats
- Gender-specific considerations for fasting (understandable for all coaches)
- When metabolic concerns require medical referral
- How to coach these interventions without creating obsession or fear
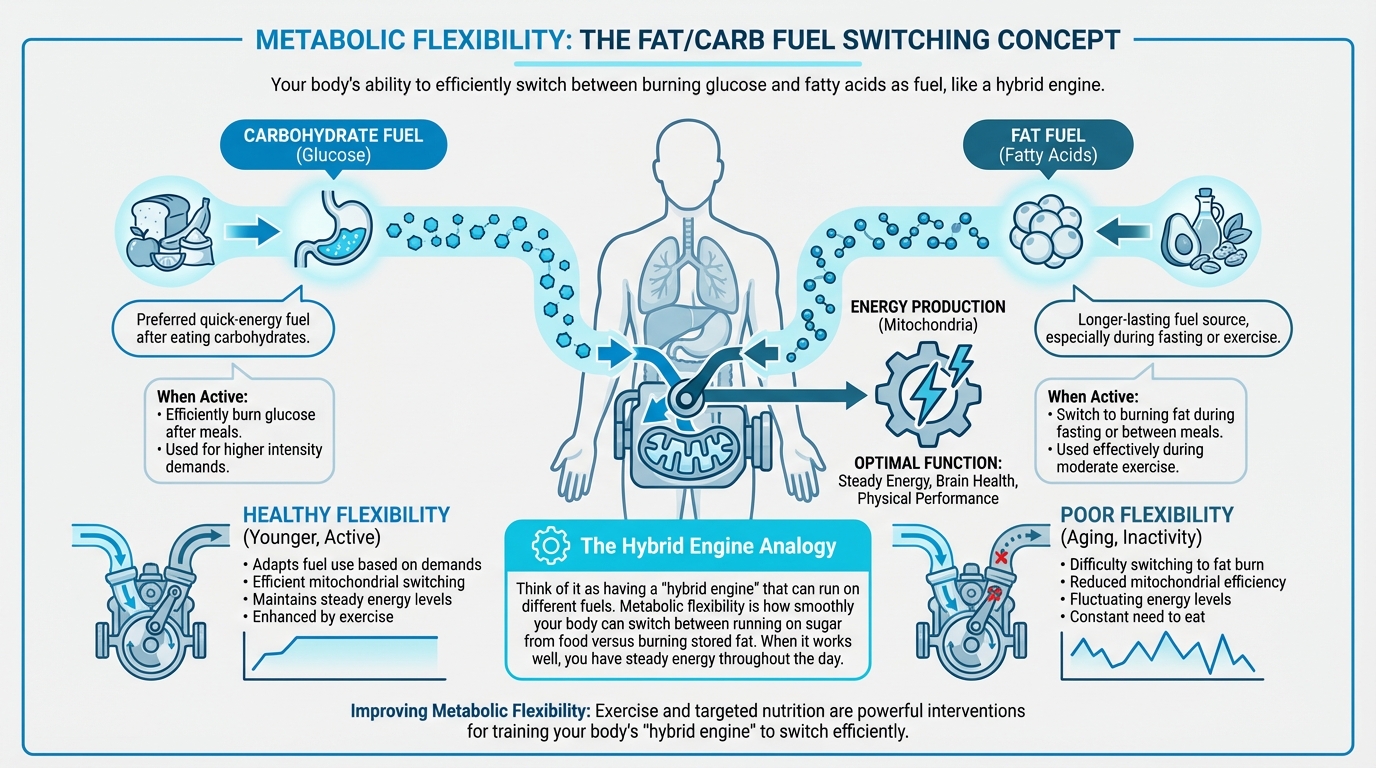
Figure: Fat/carb fuel switching concept
The big idea: This chapter is about when and how to eat. Complementing Chapter 2.7's focus on what to eat. Meal timing and metabolic health are real factors in longevity, but they're often overhyped in optimization culture. Here, we'll separate evidence from enthusiasm, give you practical strategies that work, and keep you firmly within coaching scope. The hierarchy matters: fundamentals first, timing optimization second.
[CHONK: Introduction: Why Meal Timing Matters (and Why It's Not Magic)]
Introduction: It's Not Just What You Eat¶
"I'm doing 16:8 fasting for longevity." "I bought a CGM to optimize my metabolism." "Should I be worried about glucose spikes?"
Clients come with a lot of ideas about meal timing: some useful, some overhyped. This chapter helps you sort the signal from the noise.
In Chapter 2.7, we covered what to eat. This chapter covers when to eat and how to support metabolic health. The bottom line: timing matters, but fundamentals matter more.
The Hierarchy: What Actually Matters¶
Here's the priority order (and it's not negotiable):
Essential (must be in place first):
- Adequate protein distributed across meals (Chapter 2.7)
- Sufficient vegetables and fiber
- Adequate sleep (Chapter 2.11)
- Regular movement (Chapter 2.9)
Valuable (add once essentials are solid):
- Post-meal walks for blood sugar management
- Pairing protein/fat/fiber with carbohydrates
- Basic overnight fasting (12 hours, which most people already do)
Advanced/Individual (fine-tuning for those with fundamentals dialed):
- Extended time-restricted eating windows (14-16 hours)
- Detailed blood sugar tracking
- Metabolic flexibility protocols
This hierarchy matters. If someone's eating processed foods for most meals, skipping breakfast won't save them. If someone's sleeping poorly and sedentary, extending their fasting window won't compensate. Fundamentals first.
What This Chapter Covers vs. What It Doesn't¶
We will cover:
- Metabolic health concepts coaches can explain to clients
- Practical strategies (post-meal walks, meal composition, timing)
- Time-restricted eating with honest evidence assessment
- Gender-specific considerations without over-medicalizing
- Clear scope boundaries for metabolic health coaching
We won't cover:
- Extended fasting protocols (24+ hours). Insufficient evidence, medical territory
- Detailed metabolic disease management. Scope of dietitians and physicians
- Specific supplement protocols for metabolic health (beyond scope of this chapter)
- Dramatic claims about "metabolic magic"
The Evidence Reality Check¶
Here's an honest assessment of what we know:
| Intervention | Evidence Quality | Reality |
|---|---|---|
| Post-meal walks | Moderate-Strong | Simple, accessible, good evidence for reducing glucose spikes |
| Protein with carbs | Moderate | Slows digestion, reduces glucose spikes |
| 12-hour overnight fast | Moderate | Most people basically do this anyway; reasonable starting point |
| Extended TRE (16:8) | Moderate | Benefits appear modest; much effect likely from calorie reduction |
| CGM for non-diabetics | Limited | Interesting data but unclear clinical significance |
| Extended fasting (24h+) | Preliminary | Autophagy benefits mostly from animal studies |
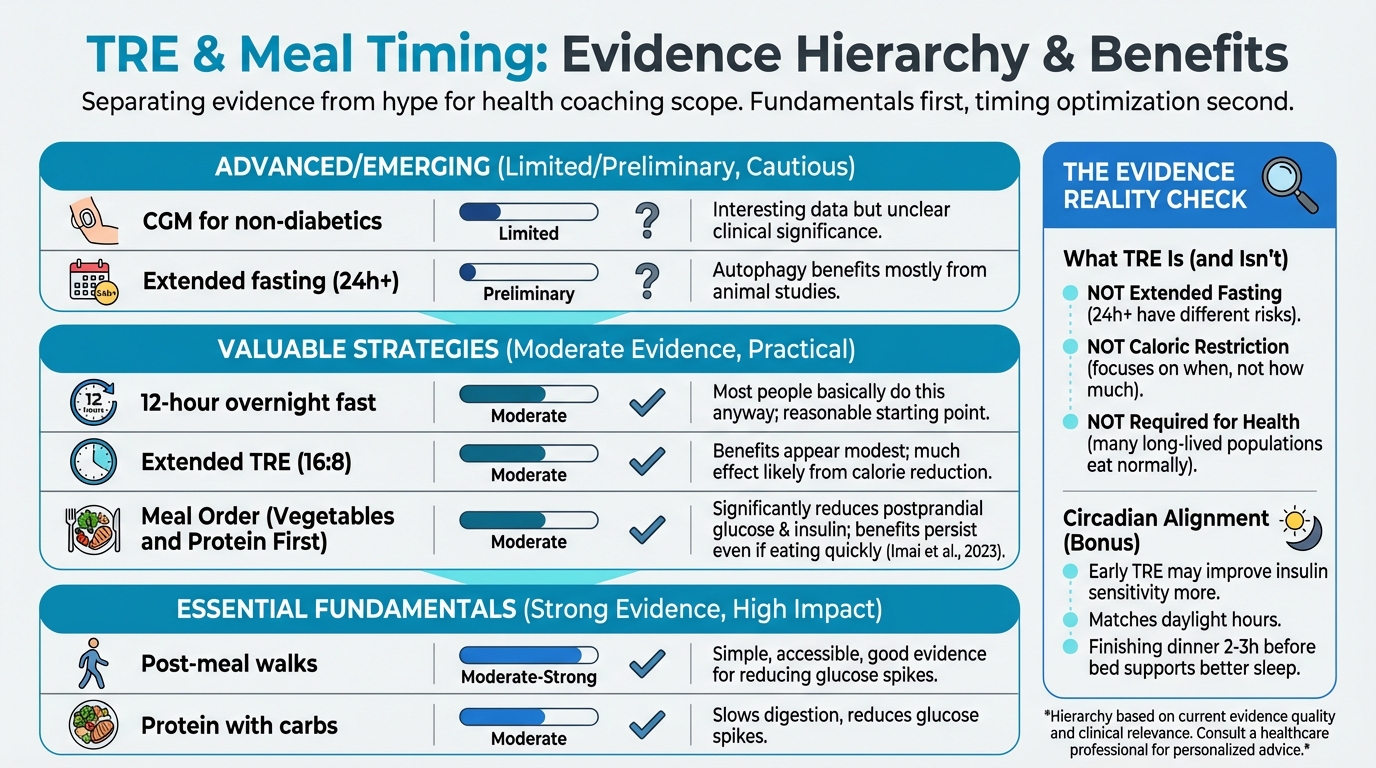
Figure: TRE benefits with evidence strength
Keep this table in mind as we proceed. We're presenting useful strategies, not metabolic miracles.
[CHONK: Understanding Metabolic Health]
Understanding Metabolic Health¶
Clients often tell you they want to “improve their metabolism” or “optimize metabolic health,” which is totally fair. The catch is that those phrases can mean very different things depending on who’s using them. In this section, we’ll define what they mean in practical, coach-friendly terms so you can explain it clearly and recognize when a concern may be drifting into medical territory. We’ll keep it practical for coaching.
What Is Metabolic Health?¶
Metabolism refers to all the chemical processes that convert food into energy and building blocks for cells. Metabolic health is basically how well those systems are working, especially how the body regulates blood sugar, stores and uses fat, and maintains overall energy balance.
If that definition feels a little clinical, that’s normal, and you don’t need to be a biochemist to coach effectively here; a few good anchors go a long way.
Clinically, metabolic health is often assessed through five markers. When three or more markers fall outside healthy ranges, that pattern is called metabolic syndrome, which is a cluster of conditions that increase risk for heart disease, stroke, and type 2 diabetes:
| Marker | Healthy Range | Risk Threshold |
|---|---|---|
| Waist circumference | <35" women, <40" men | Above these |
| Triglycerides | <150 mg/dL | ≥150 mg/dL |
| HDL cholesterol | >50 women, >40 men | Below these |
| Blood pressure | <130/85 mmHg | ≥130/85 mmHg |
| Fasting glucose | <100 mg/dL | ≥100 mg/dL |
Scope note: Coaches cannot diagnose metabolic syndrome, and you also shouldn’t be interpreting labs the way a clinician would. Still, knowing these markers helps you spot potential red flags and make a timely referral when needed. That’s part of good coaching: knowing your lane.
Metabolic Flexibility: The Core Concept¶
Metabolic flexibility is your body's ability to switch between different fuel sources depending on what's available. You can think of it like having a “hybrid engine” that runs smoothly on more than one fuel:
- Glucose (from carbohydrates): Your body's preferred quick-energy fuel
- Fatty acids (from stored fat): A longer-lasting fuel source, especially during fasting or exercise
A metabolically flexible person can:
- Burn glucose efficiently after a higher-carb meal, then shift toward fat burning between meals or during fasting.
- Use fat effectively during moderate exercise, and adjust fuel use as energy demands change.
Why Metabolic Flexibility Matters for Aging¶
Research shows that metabolic flexibility tends to decline with age, and it usually happens through a few overlapping mechanisms:
Mitochondrial changes: Your mitochondria (the cellular “power plants” that produce energy) become less efficient at switching between fuel sources. Studies show that aging reduces activity of CPT1B, a key enzyme for fat oxidation, making it harder for older muscles to burn fat under lipid load (Vieira-Lara et al., 2021).
Insulin resistance: With age, cells often become less responsive to insulin's signal to take up glucose, which can make it harder to clear blood sugar after meals and can shift metabolism toward more constant glucose burning rather than flexible fuel switching.
Sedentary effects: Inactivity compounds age-related changes, which is why exercise is such a big deal for maintaining metabolic flexibility. It trains mitochondria to switch efficiently between fuels, and the good news is that this is something clients can work on.
Signs of Poor Metabolic Flexibility¶
Clients with reduced metabolic flexibility may experience:
- Energy crashes between meals (can't access stored fat efficiently)
- Carbohydrate dependency (feeling like they "need" carbs to function)
- Difficulty fasting even for short periods without feeling terrible
- Afternoon slumps despite adequate sleep
- Weight gain concentrated around the midsection
These aren’t diagnostic, and lots of factors can cause these symptoms. Still, they’re useful conversation-starters for exploring eating patterns, activity, sleep, stress, and whether a referral might be appropriate.
The Good News: Exercise Restores It¶
Here’s the headline: Exercise is the most powerful intervention for metabolic flexibility (Pan et al., 2025). More specifically, different exercise modes tend to shine in slightly different ways:
- Resistance training often ranks highest for improving overall insulin sensitivity, while cycling tends to rank best for lowering fasting glucose.
- Combined aerobic and resistance programs also work well, and they effectively lower insulin resistance markers.
This connects directly to Chapter 2.9 (Exercise), because the most reliable way to support metabolic health usually isn’t a meal-timing trick. It’s regular movement, done consistently. It’s simple in concept, but not always easy in practice.
The Build/Repair Connection¶
Remember from Chapter 2.7 that your cells toggle between “build mode” (after eating) and “repair mode” (during fasting), and meal timing can influence that rhythm.
Constant snacking tends to keep you in build mode all day, while an overnight fast gives repair mode some space to happen. That’s the basic science behind time-restricted eating, though the effects in humans are modest, not miraculous. It’s not magic; it’s just biology.
For the full biochemistry, see How Food Affects Aging Biology.
Coaching in Practice: Explaining Metabolic Flexibility¶
Client: "What does 'metabolic flexibility' even mean? I keep hearing about it."
Coach: "Totally fair. Think of your body like a hybrid car: it can run on either gasoline or electricity. Metabolic flexibility is how smoothly you switch between burning sugar from food and burning stored fat. When that switch works well, energy tends to feel steadier. When it doesn’t, people often feel like they have to eat constantly just to function."
Client: "That sounds like me. I crash if I don't eat every few hours."
Coach: "That’s really common, so you’re not alone. It often improves with exercise and overall activity level. The single best thing we can do for metabolic flexibility is exercise, because it trains your system to switch fuels more smoothly."
[CHONK: Blood Sugar Management]
Blood Sugar Management: Practical Strategies¶
Blood sugar regulation connects directly to aging biology. Chronic high blood sugar accelerates glycation (sugar molecules damaging proteins), promotes inflammation, and contributes to insulin resistance, all hallmarks of aging.
The good news is that you don't need perfect blood sugar to age well. You just need reasonable blood sugar management through simple, sustainable habits, and this section covers evidence-based strategies coaches can implement within scope.
Why Blood Sugar Matters for Longevity¶
The connection between blood sugar and aging is well-established:
- Higher fasting glucose predicts higher risk of chronic disease and death over time
- Centenarians consistently show better blood sugar control than the general population, which may help explain their longevity
- Post-meal spikes seem to drive more damage than modest sustained elevation
The practical implication: Strategies that reduce post-meal glucose spikes, even modestly, support healthier aging. You don't need perfection, just reasonably good patterns.
Strategy 1: Post-Meal Walks¶
The most consistently supported intervention for blood sugar is simple: take a walk after eating.
Multiple studies confirm this works: walking after meals reduces blood sugar significantly better than walking before meals or not walking at all, and even 10 minutes can make a measurable difference. Effects are strongest after dinner, when overnight glucose matters most.
Why it works: Walking activates your muscles, which pull sugar directly from your bloodstream without needing insulin. It's like opening a drain.
How to implement:
- Minimum: 10 minutes of easy walking after a meal, even at a relaxed pace
- Better: 15-20 minutes at a moderate pace (you can still hold a conversation)
- Timing: Start within an hour of eating; sooner is usually better
- Priority meal: If you only pick one, choose dinner
Coaching in Practice: Post-Meal Walks¶
Client: "I don't have time for a walk after every meal."
Coach: "It doesn't have to be formal 'exercise'; it can be everyday movement like walking the dog, taking the stairs, or parking farther away. Even 10 minutes after dinner, when it matters most, can make a real difference for blood sugar."
Client: "Just 10 minutes?"
Coach: "Yep, that's enough to get your muscles pulling sugar out of your bloodstream; the goal is movement, not performance."
Strategy 2: Meal Order (Vegetables and Protein First)¶
Eating vegetables and protein before carbohydrates reduces postprandial glucose spikes. It's a simple reordering of what's already on your plate.
What the evidence shows:
A 2024 randomized crossover trial in gestational diabetes found that eating vegetables first, then protein, then carbohydrates reduced:
- 60-minute postprandial glucose by ~5.9% and 120-minute postprandial glucose by ~6.1%
- Insulin response by ~8-11%
(Murugesan et al., 2024)
In healthy young women, eating vegetables first significantly reduced postprandial glucose and insulin at 30 and 60 minutes, and benefits persisted even when meals were eaten quickly (Imai et al., 2023).
How it works:
Vegetables and protein slow gastric emptying: the rate at which food leaves your stomach. When carbohydrates arrive more slowly in your small intestine, glucose enters your bloodstream more gradually, reducing the spike.
Practical implementation:
- Start meals with a salad or vegetable side, even if it's just a few bites
- Eat protein early in the meal (or at least alongside the vegetables)
- Save starchy carbohydrates and bread for mid-to-late in the meal
- Don't obsess; the general pattern matters more than precise sequencing
Strategy 3: Avoiding "Naked Carbs"¶
"Naked carbs" are carbohydrates eaten alone without protein, fat, or fiber. Think: a plain bagel, a handful of crackers, juice without anything else.
When carbohydrates are eaten alone, they're digested quickly, causing rapid blood sugar spikes. Pairing carbs with protein, fat, or fiber slows this process.
What the evidence shows:
A 2024 Frontiers in Nutrition study found that protein-rich, lower-carbohydrate meals produced smaller postprandial glucose peaks and lower glucose area-under-curve than iso-caloric high-carbohydrate or high-fiber meals (Ekberg et al., 2024).
A 2022 Nutrients review confirmed that adding protein or fat to carbohydrate meals slows gastric emptying, and viscous soluble fibers (like psyllium, pectin, or beta-glucan) slow carbohydrate absorption, both attenuating glucose spikes.
Practical implementation:
- Apple → If you're having an apple, add almond butter for fat, which slows absorption.
- Toast → Top toast with eggs (or another protein) to help blunt the spike.
- Rice bowl → Build rice bowls with chicken and vegetables, so carbs come with protein and fiber.
- Crackers → Pair crackers with cheese and some vegetables to add protein and more volume.
- Smoothie → In smoothies, include protein powder or Greek yogurt so it's not just fruit.
Coaching in Practice: "Dress Your Carbs"¶
Client: "Should I avoid carbs for blood sugar?"
Coach: "You don't have to avoid carbs. Instead, try not to eat them 'naked', meaning on their own, and pair them with protein, fat, or fiber."
Client: "Like what?"
Coach: "Apple with almond butter instead of just an apple; toast with eggs instead of just toast; rice with chicken and vegetables instead of just rice. It slows digestion and smooths out your blood sugar, so it's the same foods, just smarter combinations."
CGM Data: A Brief Mention¶
Continuous glucose monitors (CGMs) are devices that track blood sugar in real time. They're increasingly marketed to non-diabetic "wellness" consumers.
What coaches should know:
CGM data can reveal individual glucose responses to different foods, meals, and activities. For motivated clients, CGM can be an interesting educational tool to:
- See how different foods affect their blood sugar, rather than relying on averages
- Notice the impact of post-meal walks or other movement in real time
- Identify patterns (e.g., higher glucose after late-night meals), then test simple changes
However:
- Evidence for CGM improving hard outcomes (cardiovascular events, mortality) in non-diabetics is limited and preliminary (Ahmed et al., 2025; Wilczek et al., 2025)
- There's also a real risk of obsession, like constantly checking numbers, feeling anxious about "spikes," or avoiding foods unnecessarily
- Individual glucose readings vary for many reasons; focusing on single values can be misleading
Scope boundaries:
- CAN: Help clients notice patterns, correlate behaviors with glucose trends
- CANNOT: Interpret clinical significance of readings, diagnose conditions, recommend treatment
Coaching in Practice: "Should I Get a CGM?"¶
What NOT to do:
- Use CGM data to diagnose a condition or set medical glucose targets
- Push clients to chase "perfect" readings, which can create anxiety and rigid eating
Client: "I've been seeing ads for CGMs. Should I get one to improve my glucose?"
Coach: "They can be interesting as a learning tool, since you'll see how walking after dinner really does flatten your glucose curve, but I'd be cautious about getting too focused on the numbers."
Client: "Why cautious?"
Coach: "The evidence that CGM improves long-term health for people without diabetes is still pretty limited, and some people get anxious chasing perfect readings. If you want to try it for a few weeks to see patterns, that's fine. Just remember the goal is building sustainable habits, not perfecting every glucose spike."
[CHONK: Time-Restricted Eating]
Time-Restricted Eating: Evidence Without Hype¶
Time-restricted eating (TRE) is one of the most discussed, and most overhyped, topics in longevity. Here’s what we actually know, and what we still don’t.
What TRE Is (and Isn't)¶
Time-restricted eating means limiting food consumption to a specific window each day, typically 8-12 hours, and fasting for the remainder.
Common protocols:
- 12:12 = a 12-hour eating window (e.g., 7am-7pm), which is a realistic baseline for many clients
- 14:10 = a 14-hour fast with a 10-hour eating window, often by finishing dinner a bit earlier and delaying breakfast slightly
- 16:8 = a 16-hour fast with an 8-hour eating window, which can work well for some people but tends to take more planning
TRE is NOT:
- Extended fasting: 24+ hour fasts are different, with different evidence and risks
- Caloric restriction: TRE focuses on when you eat, not how much (though people often eat less with shorter windows)
- Required for health: Many healthy, long-lived populations eat normally without specific time restrictions
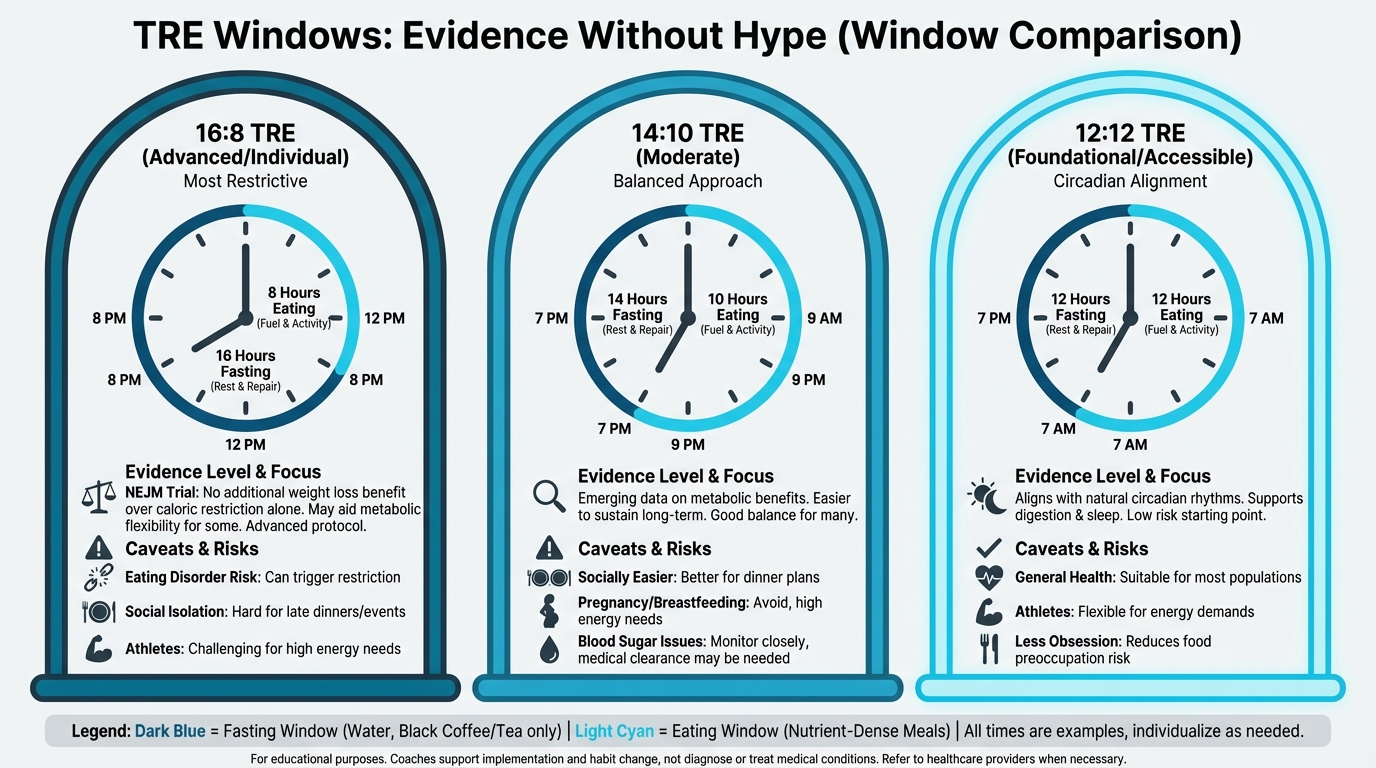
Figure: Different eating windows (16:8, 14:10, 12:12) with evidence levels
The Evidence: Modest Benefits, Likely From Calorie Reduction¶
The research points to a pretty consistent theme: TRE can help, but the effects are usually modest, and they often come from eating fewer calories overall.
Weight and body composition:
TRE consistently produces modest weight loss (about 1-2 kg) compared to unrestricted eating, and several meta-analyses confirm this:
- TRE alone vs. no restriction: weight -1.59 kg, fat mass -0.93 kg (IJBNPA, 2025)
- TRE in overweight/obese women: weight -1.93 kg (Frontiers in Nutrition, 2025)
- TRE combined with exercise: additional -1.86 kg vs. exercise alone (Advances in Nutrition, 2024)
But here’s the catch:
A high-quality New England Journal of Medicine trial found that adding TRE to prescribed calorie restriction did not increase weight loss beyond calorie restriction alone (JAMA summary, 2023). In other words, when calories are controlled, the timing window itself doesn’t add extra benefit.
So a lot of TRE’s “magic” is probably just calorie reduction in disguise. That can feel a little anticlimactic, but it also means you have options.
Glycemic and metabolic markers:
- Frequent reductions in fasting insulin and insulin resistance markers (HOMA-IR, a calculation using fasting glucose and insulin to estimate insulin resistance)
- Some studies show improved HbA1c (a measure of average blood sugar over 2-3 months) in metabolic syndrome (1.7% greater reduction vs. control in one RCT)
- Effects on fasting glucose and lipids are inconsistent across studies
Circadian alignment:
Early time-restricted eating (eating earlier in the day and finishing dinner early) may provide additional benefits:
- Some studies show early TRE improves insulin sensitivity more than late TRE
- Eating aligned with daylight hours, and finishing dinner 2-3 hours before bed, matches circadian biology and can support sleep and overnight metabolism
Lean mass concerns:
Overall, analyses generally show no significant lean mass loss with TRE, though a few report small reductions (~0.5 kg). Adequate protein and resistance training likely mitigate any losses.
The Protocol: 12-16 Hour Overnight Fasts¶
Based on the evidence, a reasonable approach looks like this.
Starting point: 12 hours
Most people essentially do this already. For example, if you finish dinner at 7pm and eat breakfast at 7am, that’s a 12-hour fast, and it’s a sensible baseline that aligns with natural eating patterns.
Extension: 13-14 hours
For clients interested in extending their window, 13-14 hours is well-tolerated by most people:
- Dinner at 7pm, breakfast at 8-9am
- Or breakfast at 8am, dinner finished by 6-7pm
Advanced: 16 hours (16:8)
A 16:8 window (e.g., noon-8pm eating) can be a reasonable experiment for clients who have solid nutrition fundamentals in place, tolerate extended fasting well, aren’t prone to food preoccupation, and don’t have medical contraindications.
Even then, protein targets still matter, and getting enough protein in a short window can be challenging.
The focus: When you stop eating
For most clients, the most practical place to start is dinner timing: finish dinner 2-3 hours before bed, stop snacking after dinner, and let overnight fasting happen naturally.
Who Benefits, Who Should Be Cautious¶
May benefit from TRE:
- Those with solid nutrition fundamentals already in place who want a little more structure, especially around late-night snacking
- Those who want simpler meal timing, including people who naturally aren’t hungry in the morning
Caution or avoid TRE:
- History of eating disorders, or anyone who notices TRE increases anxiety or food preoccupation (TRE can trigger restrictive patterns)
- Athletes with high energy demands, and pregnant or breastfeeding clients, since it can be hard to meet elevated energy needs in short windows
- Blood sugar issues requiring frequent eating (some people with diabetes need regular meals)
- Clients on diabetes medications, since medication timing may need adjustment (medical referral)
The Honest Framing: One Tool, Not THE Tool¶
Here’s a clean way to frame TRE: it’s a tool that can create helpful structure (especially for late-night snacking), but it doesn’t replace the fundamentals.
Coaching in Practice: When 16:8 Makes Sense¶
Client: “Okay, I’ve been hitting my protein targets for a month now, so can I try extending my fast?”
Coach: “Yep, that can be a reasonable next step. Here’s a simple experiment: Finish dinner by 7pm and don’t eat until 9am, which gives you a 14-hour fast. Try it for a week and see how your energy, hunger, training, and sleep respond.”
Client: “And if that feels fine?”
Coach: “Then we can consider pushing toward 16 hours. But if it creates stress or makes you think about food constantly, we’ll pull it back. Health includes your relationship with food, not just metabolic markers. Choosing not to use TRE is a valid option.”
[CHONK: Gender Considerations in Fasting]
Gender Considerations in Fasting¶
Men and women can respond differently to fasting, and that isn’t about being overly cautious; it’s biology. Since you’ll likely coach clients of all genders, understanding these differences helps you tailor guidance that’s both safe and effective, and it can help clients feel less “broken” when a protocol that worked for someone else doesn’t work for them.
The Core Difference¶
In general, women’s bodies are more sensitive to energy restriction. When the body senses that not enough food is coming in, it tends to prioritize survival over reproduction, which can show up as hormonal disruption, missed periods, and other downstream effects.
This isn’t a small effect either, and studies show sustained caloric restriction is the most common trigger for menstrual irregularities in otherwise healthy women.
The practical takeaway: A fasting protocol that works fine for a male client may cause problems for a female client, so context matters.
The Exception: PCOS¶
Here’s an important detail: For women with PCOS (polycystic ovary syndrome), TRE often helps. Studies show improved menstrual regularity and better hormonal profiles. That tracks, because PCOS often involves insulin resistance, and TRE’s insulin-sensitizing effects can help normalize hormone production.
A common pattern: TRE may help women with metabolic dysfunction and hormone excess, while potentially harming women who are already lean or already running low on energy, so context matters.
Menstrual Cycle Considerations¶
For women who menstruate, the menstrual cycle can change energy needs and fasting tolerance. This isn’t about “lack of willpower.”
Follicular phase (approximately days 1-14):
- Begins with menstruation and ends at ovulation; estrogen rises while progesterone stays low
- Energy needs are relatively lower, and many women tolerate extended fasting better during this phase
- If feeling good, can try extending to 14-16 hours
Luteal phase (approximately days 15-28):
- Begins after ovulation and ends at menstruation; progesterone rises and energy needs increase
- Many women feel hungrier and have less tolerance for restriction, so limit fasting to 12-13 hours
- Priority: Adequate protein and energy. Don’t fight hunger signals
Signs of Over-Restriction¶
As you coach, keep an eye out for signs that fasting might be too aggressive, and invite clients to watch for these in themselves too. No judgment: these are data, not a character flaw.
Physical signs:
- Menstrual irregularities (missed periods, longer cycles) or other cycle changes
- Hair loss or thinning, feeling cold when others are comfortable, or persistent fatigue
- Sleep disruption, especially waking at night hungry
Psychological signs:
- Excessive preoccupation with food or eating windows, or anxiety about "breaking" the fast
- Rigid rules that create stress, or social isolation to maintain a fasting schedule
If clients report these signs, the move is usually to back off: shorten fasting windows, increase total food intake, and reduce overall restriction, because health is the goal, not “winning” fasting. You don’t have to nail the perfect window on the first try; small tweaks count.
Special Populations¶
Pregnancy: TRE is not recommended, since energy and nutrient needs are elevated and this is not the time for any form of restriction.
Breastfeeding: Extra caution is warranted because milk production requires significant energy. If TRE is practiced at all, windows should be minimal (12 hours maximum) and adequate calories ensured.
Perimenopause: Responses are highly individual. Some women do well with TRE, while others find it exacerbates symptoms (sleep disruption, mood changes). Start conservative, then adjust based on response.
Post-menopause: Generally well-tolerated. Without menstrual cycle considerations, post-menopausal women can experiment with TRE like anyone else, with attention to protein adequacy and overall well-being.
Practical Framing for Coaches¶
The goal is not to medicalize normal eating. The goal is to help clients use fasting (if they choose it) in a way that supports their bodies rather than battling them.
Coaching in Practice: Menstrual Cycle Considerations¶
Client: "I noticed fasting is way harder right before my period. Is that normal?"
Coach: "Yes, that’s very common. Your energy needs can shift across your cycle, especially in the second half after ovulation, when your body often needs more energy. Feeling hungrier there is a normal signal."
Client: "So should I stop fasting during that time?"
Coach: "You don’t necessarily have to stop, but I wouldn’t fight your body either. During the luteal phase, a 12-13 hour fast tends to feel more doable for many women. Then, if you want to experiment with longer windows, the follicular phase, before ovulation, is often when people tolerate it better."
Client: "Okay, so I can flex it based on how I feel?"
Coach: "Exactly. We can use your cycle and your symptoms as feedback, not a rule you have to “obey.”"
Coaching in Practice: For Coaches Working With Female Clients¶
Client: (reports missed periods, fatigue, food preoccupation after starting fasting)
Coach: "Thanks for telling me. Those can be signs the overall restriction is too much for your body right now."
Client: "So I should stop fasting?"
Coach: "At least for the moment, I’d like us to back off and see if those symptoms settle. We can shorten your fasting window, make sure you’re eating enough overall, and check in again in a few weeks."
Client: "And if my period still doesn’t come back?"
Coach: "Then it’s worth mentioning to your doctor. And just to be clear, this isn’t you failing at fasting; it’s your body giving us useful feedback."
Key principle: When in doubt, shorter fasting windows and adequate calories are safer choices for female clients.
Energy Availability: The Key Metric¶
For women, especially active women, energy availability may matter more than fasting duration. Energy availability = (Energy intake - Exercise energy expenditure) / Fat-free mass.
Research suggests ~45 kcal/kg fat-free mass per day supports menstrual function and athletic performance (Holtzman & Ackerman, 2021).
Translation for coaches: Fasting protocols that significantly reduce caloric intake and are combined with exercise may push energy availability too low, even if the fasting window itself seems moderate. So if a client is training hard and fasting, it’s worth double-checking total intake, recovery, and cycle health.
[CHONK: Coaching Metabolic Health]
Coaching Metabolic Health: Scope and Practice¶
Metabolic health sits right at the edge of coaching scope, so some parts are clearly within bounds while others call for medical collaboration. If this section feels a little more "clinical" than usual, that’s normal; you’re dealing with real physiology and, sometimes, real risk. The goal here is to make the boundaries clear and give you practical, coach-appropriate ways to help.
Scope of Practice: Clear Boundaries¶
If you’re ever unsure, come back to this: educate, observe, support, and refer when needed. The good news is that you can still be very helpful without crossing the line.
Coaches CAN:
- Educate about metabolic health concepts (what you've learned in this chapter), and coach meal timing and meal composition strategies that support steadier energy and appetite.
- Guide TRE implementation for healthy clients while helping them notice patterns in energy, hunger, and how they respond to different foods.
- Ask questions about energy levels, hunger patterns, and eating habits, and support clients in implementing recommendations from their healthcare provider.
Coaches CANNOT:
- Diagnose insulin resistance, prediabetes, diabetes, metabolic syndrome, or other metabolic disorders, or treat those conditions.
- Interpret lab values (HbA1c, fasting glucose, lipid panels) diagnostically, or use CGM data to make clinical assessments.
- Recommend TRE for clients with an eating disorder history without medical clearance, or adjust medication timing or dosage.
The Metabolic Health Decision Tree¶
Here’s a simple decision tree you can use when a client brings up metabolic concerns or blood sugar issues. Most of the time, you’re sorting into “safe to coach” vs. “time to loop in a clinician.”
Client mentions metabolic concerns or blood sugar issues
↓
Does client have a diagnosed condition?
(diabetes, prediabetes, PCOS)
↓
┌───────YES──────┴────────NO──────────┐
↓ ↓
Is client working with Are there warning signs?
a medical provider? (see list below)
↓ ↓
┌──YES────┴───NO────┐ ┌────YES───┴────NO────┐
↓ ↓ ↓ ↓
Support their Refer to Refer to OK to coach
medical plan medical medical general
(within scope) provider provider strategies
Warning signs requiring referral:
- HbA1c >5.7% (prediabetes threshold. HbA1c measures average blood sugar over 2-3 months) or fasting glucose consistently >100 mg/dL.
- Client reports “blood sugar crashes,” severe symptoms, or other blood-sugar-related episodes that feel hard to manage.
- Signs of metabolic syndrome (multiple markers. See earlier table).
- Significant unexplained weight changes, especially if they’re rapid or ongoing.
- Client uses blood sugar-affecting medications, or has a history of eating disorders (needs clearance before any fasting approach).
Assessment Approaches (Within Scope)¶
You can learn a lot just by talking with clients and listening for patterns over time. You’re not diagnosing anything here, but you are paying attention to what’s happening in their day-to-day experience, which is exactly right.
Questions about energy patterns:
- "How does your energy feel throughout the day, and do you tend to crash if you go a few hours without eating?"
- "What happens if you miss a meal, and do you ever wake up at night hungry?"
Questions about eating patterns:
- "Walk me through a typical day of eating, including when you have your first and last food of the day."
- "Do you snack frequently, what usually prompts that, and how do you feel after different types of meals?"
Observations (not diagnoses):
- Client reports energy crashes → may benefit from steadier-meal and blood sugar-support strategies.
- Client eats most calories at dinner → could try shifting more of that intake earlier in the day.
- Client snacks constantly → may benefit from more satisfying meals, especially with adequate protein and fiber.
- Client reports carb cravings → ensure adequate protein and regular meals first, then adjust meal composition as needed.
Building Sustainable Patterns¶
Your coaching approach for metabolic health is the same behavior-change approach you’d use anywhere else: start simple, build consistency, and adjust based on what the client notices.
Start with fundamentals:
Before any timing optimization, ensure:
- Adequate protein at meals (Chapter 2.7), ideally spread across the day.
- Sufficient vegetables and fiber to support fullness and digestion.
- Minimized ultra-processed foods most of the time, especially the ones that trigger overeating.
- Regular meals (not constant snacking, not skipping meals), so the client has a predictable rhythm.
Add structure, not rigidity:
- Aim for consistent meal times (a rough schedule is enough), and keep an easy overnight fast of about 12 hours.
- When it fits the client’s life, add post-meal movement, like a short walk.
Progress based on response:
- If fundamentals are solid and the client is interested, try extending the overnight fast.
- Monitor how the client feels, not just numbers.
- Adjust based on feedback (energy, mood, sleep, hunger).
Avoiding Orthorexia and Restriction Anxiety¶
Orthorexia is an unhealthy obsession with "healthy" eating, and metabolic health interventions can unintentionally trigger this in susceptible clients. If you’re thinking, "Wait, how do I support metabolic health without making things worse?" you’re asking the right question.
Watch for:
- Rigid timing rules that create stress ("I can't eat until exactly noon") or anxiety if the eating window is “broken.”
- Social isolation to maintain eating patterns, or avoiding events because they don’t fit the plan.
- Escalating restriction ("16 hours isn't enough, I need 20") and a growing sense that “more strict” is always better.
- Food and blood sugar numbers becoming the primary focus of life, including perfectionism about CGM/"spikes."
Your response:
- Validate the client’s interest in health, and gently explore whether the approach has started to feel intense or all-or-nothing.
- Emphasize flexibility and sustainability over “perfect” optimization, and remind them that occasional variations don’t matter in the big picture.
- If the pattern feels concerning (rigidity, anxiety, escalating restriction), refer for psychological support.
Coaching in Practice: When TRE Creates Stress¶
What NOT to do
Client: "I broke my fast early yesterday and I felt terrible about it all day."
Coach: "You can’t do that if you want results. You need to be more disciplined and stick to the plan."
That kind of response usually adds shame and tightens the rules, which can make the stress spiral worse.
A better approach
Client: "I broke my fast early yesterday and I felt terrible about it all day."
Coach: "Thanks for telling me. I’m noticing something: you seem more stressed about your eating window than you were before we started this. If this approach is making you think about food more, not less, it’s not working."
Client: "But I want to get the longevity benefits..."
Coach: "I hear you, and health includes your relationship with food, not just metabolic markers. What if we stepped back to something simpler for now? Finish dinner by 7pm, eat when you’re hungry in the morning, and focus on food quality instead of timing perfection. The anxiety costs more than the benefits."
Case Study: Client Wanting to "Optimize Metabolism"¶
Sarah, 42, comes to you wanting to "optimize her metabolism." She’s read about intermittent fasting, metabolic flexibility, and glucose optimization. She has a CGM and tracks everything.
Assessment reveals:
- Already eating adequate protein (good)
- Exercises 4x/week including strength training (good)
- Sleeps 6 hours/night (concern)
- Very anxious about glucose "spikes" on CGM
- Has restricted eating window to 6 hours daily
- Feeling tired and irritable
If you’ve coached a client like Sarah, you know how easy it is for "health tools" to turn into "health pressure."
The coaching approach:
Step 1: Identify the real issue
Sarah’s fatigue and irritability may be from under-eating (a 6-hour window makes adequate nutrition hard) and poor sleep, not suboptimal metabolism.
What NOT to do
Coach: "Your CGM says you’re spiking. Let’s tighten your eating window even more and cut carbs further."
That approach can reinforce restriction and anxiety while missing the more likely drivers of how Sarah feels.
Step 2: Redirect focus with a real conversation
Coach: "Sarah, I can tell you’ve put a lot of effort into this. Before we change anything, can I ask a couple quick questions?"
Sarah: "Sure. I just really want to optimize this."
Coach: "I hear you, and looking at your week, you’re strength training four times, you’re hitting protein, and you’re tracking with a CGM. What stands out to me is sleep. You’re averaging about 6 hours a night, right?"
Sarah: "Yeah. I’m usually up late, then I wake up early."
Coach: "That matters, because your sleep at 6 hours is probably affecting your metabolism more than your eating window. I’m also noticing how stressful the CGM feels for you, and that stress itself affects blood sugar."
Sarah: "So you think I’m doing the wrong thing with fasting?"
Coach: "I think you’re working hard, and the plan might be costing you more than it’s giving you right now. What if we simplified for a few weeks: extend your eating window back to 8-10 hours so it’s easier to get enough food and hit protein targets, prioritize getting to 7-8 hours of sleep, and put the CGM away for a bit. Then we’ll see how you feel."
Sarah: "Honestly, taking a break from the CGM sounds like relief."
Coach: "That’s useful data in itself. How about we try that for a couple of weeks, and keep it flexible?"
Step 3: Monitor response
- Over the next couple of weeks, did her energy improve and was she recovering better from training?
- Did her anxiety around food and CGM numbers decrease, and was she enjoying food more while thinking about it less?
[CHONK: Deep Health Integration]
Deep Health Integration¶
Metabolic health touches every dimension of Deep Health. Here's how:
Physical¶
Most of this chapter sits in the physical dimension, since blood sugar regulation, metabolic flexibility, body composition, and energy production all live here. The interventions we've discussed—post-meal walks, meal composition, reasonable TRE—support metabolic function in very direct, practical ways.
Coaching example: choosing one lever to start¶
What NOT to do
Client: “Where should I start for better metabolic health?”
Coach: “All of it. Walk after every meal, change your macros, and do TRE starting tomorrow.”
Better
Client: “Where should I start for better metabolic health?”
Coach: “How about we pick one lever that fits your life this week? For many people, a 10-minute walk after dinner is a simple place to start, and we can build from there.”
Mental¶
Brain function depends on glucose regulation. Your brain uses about 20% of your glucose, which means it’s sensitive to blood sugar that runs too high or dips too low. If you’ve ever felt “hangry” or foggy, you’ve felt this firsthand.
- When blood sugar stays steadier, most people notice better focus and clearer thinking.
- When glucose swings up and down, it’s common to feel foggy and struggle to concentrate.
- Over the long term, better glycemic control is linked to a lower risk of cognitive decline.
The MIND diet connection from Chapter 2.7 applies here too, because what you eat and when you eat it can affect brain health.
Coaching example: linking symptoms to patterns¶
What NOT to do
Client: “I crash hard around 3 pm. Should I try a longer fast?”
Coach: “Probably. Just push through it and drink coffee.”
Try this instead
Client: “I crash hard around 3 pm. Should I try a longer fast?”
Coach: “Maybe, but we can start with what we can see. What did lunch look like, and what do you notice about your energy 2–3 hours later?”
Emotional¶
Your relationship with food is part of health. This is also where “metabolic optimization” can accidentally slide into something that doesn’t feel good day to day.
If metabolic interventions start to create anxiety about eating windows, fear of “bad” foods, guilt about glucose spikes, or rigid rules that remove the enjoyment of eating, then they’re harming emotional health, even if they’re “improving” metabolic markers. Balance matters, too.
Coaching example: keeping markers in perspective¶
What NOT to do
Client: “I feel guilty every time my glucose spikes.”
Coach: “Then you need to tighten your rules until it stops happening.”
Better
Client: “I feel guilty every time my glucose spikes.”
Coach: “Thanks for saying that out loud. The goal is information, not judgment. What would a ‘good enough’ approach look like that supports your health and still lets you enjoy eating?”
Social¶
Eating is fundamentally social, so part of good coaching here is building in flexibility. Rigid meal timing can isolate people, for example:
- Skipping late dinners with friends because they fall outside an eating window
- Feeling anxious about eating at the “wrong” time at social events
- Disrupting family meals when everyone is on a different schedule
Occasional deviation from patterns for social eating is not just acceptable, it’s healthy. “I skip the fasting window on Sundays for family brunch” is a reasonable approach.
Coaching example: building flexibility on purpose¶
What NOT to do
Client: “My friends want to go out late, but it breaks my window.”
Coach: “Then don’t go. Consistency is the only thing that matters.”
A better approach
Client: “My friends want to go out late, but it breaks my window.”
Coach: “We can plan for it. You could keep your usual pattern most days and choose one or two ‘late dinner’ nights each week, then we’ll see how you feel and how your markers respond.”
Environmental¶
Eating aligned with circadian rhythms connects to environmental health. We’re biologically designed to eat during daylight and rest at night, while modern life (late-night eating, shift work, artificial light) can disrupt that alignment.
Client: “What are a few simple timing tweaks that won’t upend my schedule?”
Coach: “Here are a few options. You can pick one that feels realistic and try it for a week.”
- Finish eating earlier in the evening when you can
- Eat larger meals earlier in the day, if that fits someone’s schedule
- Align eating with natural light cycles as much as practical
Coaching example: keeping timing supportive (not stressful)¶
What NOT to do
Client: “I’m trying to do an 8-hour eating window, but my family eats late and it’s stressing me out.”
Coach: “You just have to stick to it. Results require discipline, so eat alone or skip dinner.”
Better
Client: “I’m trying to do an 8-hour eating window, but my family eats late and it’s stressing me out.”
Coach: “That makes sense. Before we pick a window, can we look at what matters most to you right now: the metabolic goal, family dinners, or reducing stress around food?”
Client: “Family dinners, honestly.”
Coach: “Great. Protecting that can be our anchor. For example, you might keep your usual pattern on weekdays and shift the window later once or twice a week for family meals, then we’ll see how your energy, hunger, and markers respond.”
Existential¶
What kind of relationship with food timing do you want?
You can invite clients to reflect:
- Is this something they can see themselves doing long term, or is it a short-term experiment?
- Does this fit with how they want to live, work, and connect with other people?
- Is the pursuit of metabolic optimization enhancing their life, or shrinking it?
Some clients genuinely enjoy structure and tracking, while others find it burdensome, and both responses are valid. The goal is helping clients find approaches that serve their larger life goals. Food timing isn't just a tactic for many people; it's part of how they live.
Coaching example: long-term fit¶
What NOT to do
Client: “I can do this for a month, but not forever.”
Coach: “Forever is the point. You just need more willpower.”
Better
Client: “I can do this for a month, but not forever.”
Coach: “That’s useful information. What would be sustainable for you long term, and what would make this feel like it’s adding to your life instead of shrinking it?”