Unit 2: Core Interventions—The Protocol¶
Chapter 2.9: Exercise: The Longevity Drug¶
[CHONK: 1-minute summary]
The big idea¶
If exercise were a pill, it would be the most prescribed medication in history.
The numbers are striking: people who do both cardio and strength training have roughly 40% lower risk of dying from any cause compared to those who don't exercise. That's a bigger effect than almost any drug we know of. And the benefits show up at any age, even for clients who start exercising later in life.
This chapter covers what actually matters for longevity: strength training to keep muscle as you age, Zone 2 cardio for metabolic health, and VO2 max training for cardiovascular reserve. We'll also cover how to talk about these with clients while respecting scope boundaries, focusing on support and education rather than prescribing exercise programs.
Key takeaways:
- Combined aerobic + resistance training is linked to ~40% lower all-cause mortality
- Each 1-MET increase in VO2 max is linked to 11-17% lower mortality
- Strength training 3-5x/week helps prevent sarcopenia
- Zone 2 cardio 150-300 minutes/week supports mitochondrial efficiency
- VO2 max training about 1x/week can be used for advanced optimization (Norwegian 4x4 protocol)
- Benefits occur at any age, and it's never too late to start
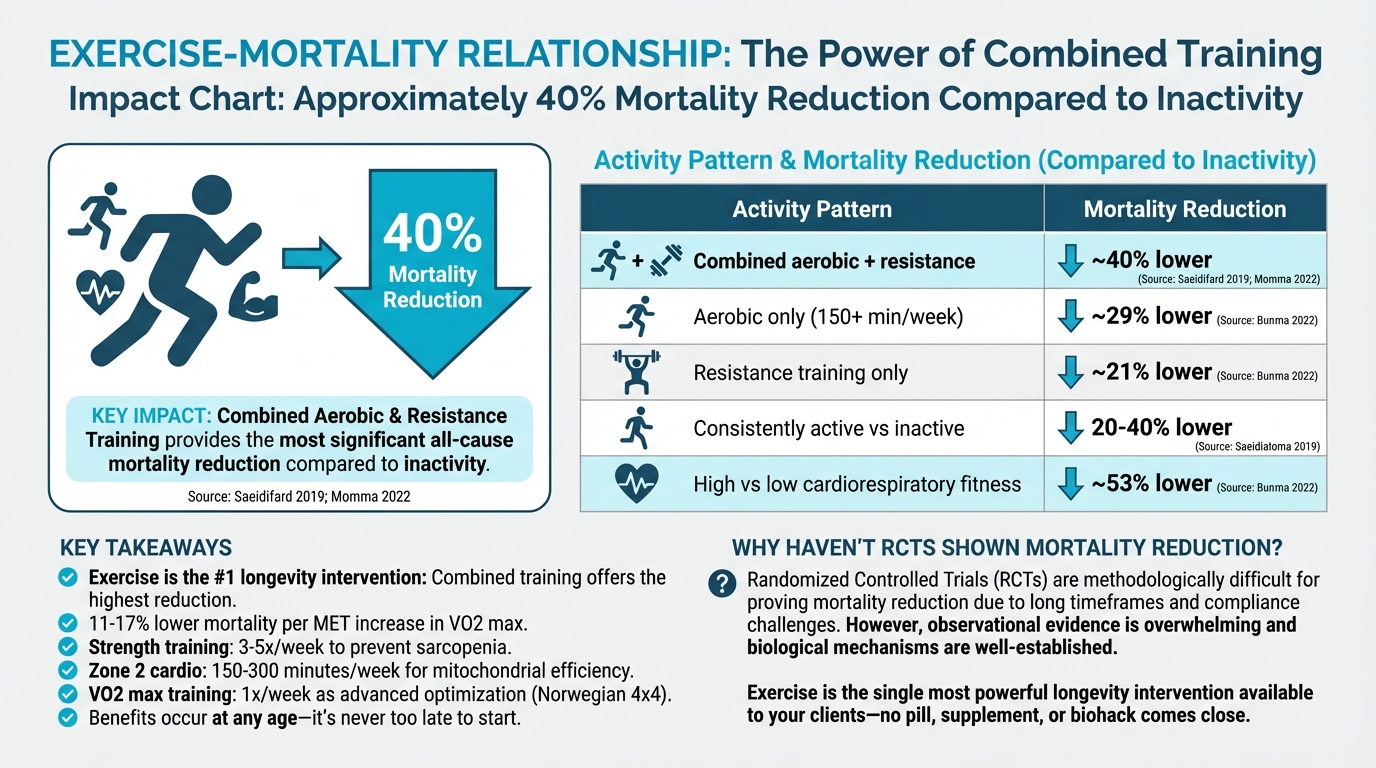
Figure: 40% mortality reduction from combined training
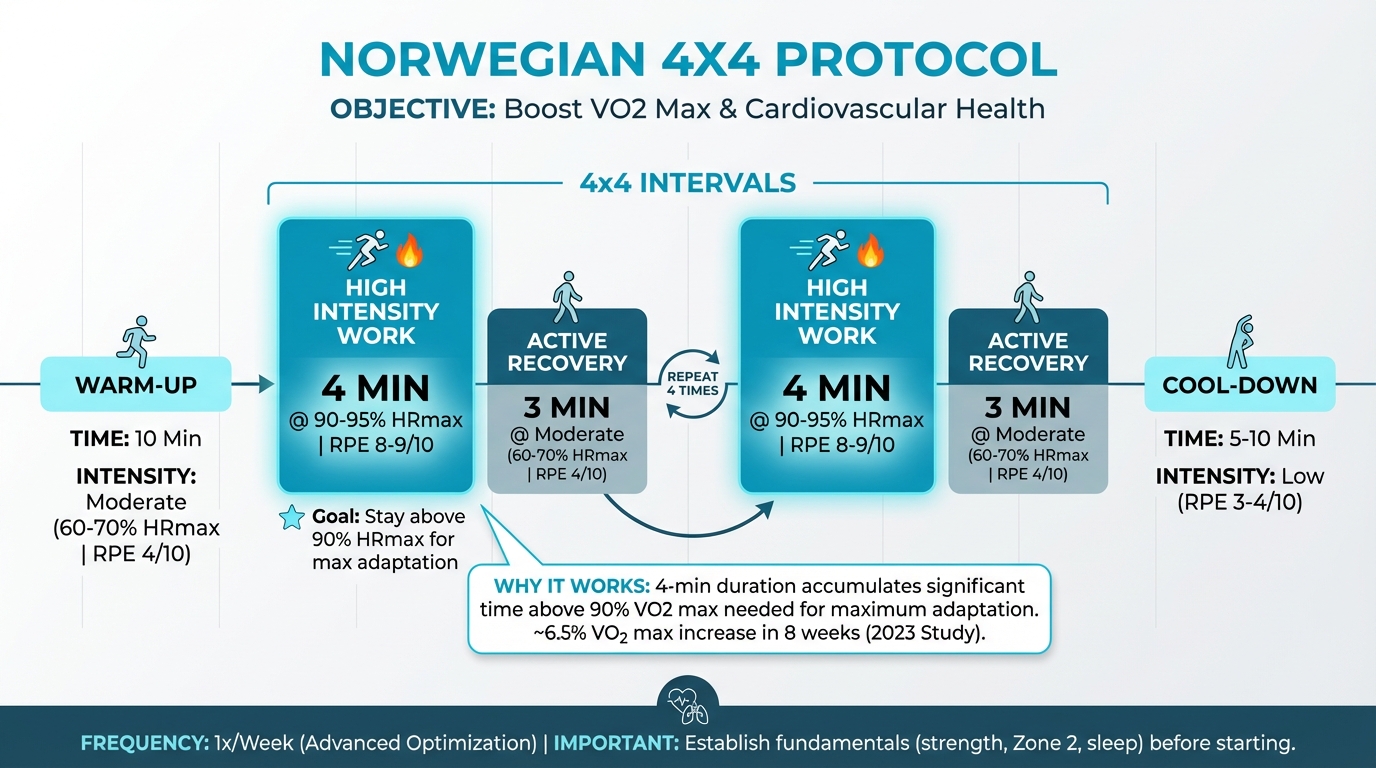
Figure: Interval structure with intensity levels
[CHONK: Section 1 - Exercise as Medicine: The Evidence]
Exercise as medicine: The evidence¶
The #1 longevity intervention¶
If exercise were a drug, it would be the most prescribed medication in history. No pharmaceutical comes close to replicating its benefits. Here's what the research shows:
Combined aerobic and resistance training reduces all-cause mortality by approximately 40 percent (HR = 0.60) compared to inactivity.[^1] That's not a typo. Doing both cardio and strength training cuts your risk of dying from any cause nearly in half.
To put this in perspective: no supplement, medication, or biohack approaches this effect size. Metformin, often discussed in longevity circles, shows modest effects in diabetic populations. Rapamycin extends lifespan in mice but lacks solid human longevity data. Exercise, meanwhile, has massive observational evidence across millions of people.
Breaking down the numbers¶
Here’s what the research actually shows:[^2][^3][^4]
| Activity Pattern | Mortality Reduction | Source |
|---|---|---|
| Combined aerobic + resistance | ~40% lower | Saeidifard 2019; Momma 2022 |
| Aerobic only (150+ min/week) | ~29% lower | Zhao 2020 |
| Resistance training only | ~21% lower | Saeidifard 2019 |
| Consistently active vs inactive | 20-40% lower | Yu 2025 meta-analysis |
| High vs low cardiorespiratory fitness | ~53% lower | Lang 2024 umbrella review |
What this tells us: Aerobic and resistance exercise each reduce mortality on their own, but combining them provides the largest benefit, so for most clients it’s not an either/or choice.
The cardiorespiratory fitness connection¶
Cardiorespiratory fitness (CRF), typically measured as VO2 max, is one of the strongest predictors of longevity we have. An umbrella review of over 20.9 million observations found:[^5]
- Each 1-MET increase in fitness is linked to 11-17% lower all-cause mortality, and high vs. low fitness is associated with approximately 53% lower mortality (HR = 0.47)
- For CVD mortality, high vs. low fitness is associated with approximately 58% lower risk (HR = 0.42)
To translate: if your client improves their fitness by just 1 MET (about 3.5 mL/kg/min of VO2 max), they meaningfully reduce their mortality risk. That's achievable with consistent training over several months.
The VILPA effect: Even small amounts matter¶
What about clients who claim they "don't have time" to exercise? The research on vigorous intermittent lifestyle physical activity (VILPA) offers hope.[^6]
In a UK Biobank study, people who accumulated just 3-4 short bouts of vigorous activity per day (totaling about 4-5 minutes) had:
- 38-40% lower all-cause and cancer mortality
- 48-49% lower cardiovascular mortality
These weren't structured workouts. They were brief bursts of vigorous activity in daily life, like running to catch a bus, climbing stairs quickly, or playing actively with children. The message: something is dramatically better than nothing, even in very small doses.
Why haven't RCTs shown mortality reduction?¶
Here's an important nuance to understand when discussing evidence with clients or colleagues: randomized controlled trials (RCTs) of exercise have not conclusively demonstrated mortality reduction.[^7]
A 2025 European Association of Preventive Cardiology scientific statement noted that pooled RCTs in older adults (≥1 year duration) showed no significant mortality effect (RR ≈ 0.95).
Why the disconnect from observational data?
Several factors explain this:
1. Duration: Most exercise RCTs run 1-3 years, and mortality benefits may require longer exposure.
2. Power: Detecting mortality differences requires massive sample sizes, which most exercise RCTs can’t realistically enroll.
3. Adherence: Even with good supervision, participants often taper their activity over time or after the study ends.
4. Control group contamination: “Control” participants often increase activity too, which shrinks the gap between groups.
This doesn't mean exercise doesn't work. It means proving mortality reduction in a controlled trial is methodologically difficult. The observational evidence remains overwhelming, and the biological mechanisms are well-established.
The occupational activity paradox¶
One curious finding: not all physical activity is created equal. High occupational physical activity (heavy manual labor) does not confer the same benefits as leisure-time exercise, and may actually increase mortality risk in men (HR ≈ 1.12).[^8]
Why? Several theories:
- Occupational activity often lacks adequate recovery
- Manual labor may not include progressive overload
- Work activity is often sustained at moderate intensity without variation
- Psychosocial stress of demanding physical jobs adds to allostatic load
The takeaway: The exercise that benefits longevity is chosen leisure-time activity with appropriate recovery, not forced physical labor without rest.
Coaching in Practice: "Does Exercise Really Matter That Much?"¶
Client: "I hear exercise is important, but does it really make that big a difference? I mean, my grandfather smoked and never exercised and lived to 85."
Coach: "The research shows that people who do both cardio and strength training have about 40% lower risk of dying from any cause compared to people who don't exercise. That's a bigger effect than almost any medication we know of."
Client: "But how do we know it's the exercise? Maybe fit people are just healthier to begin with."
Coach: "That's a fair question. The evidence comes from studies of millions of people across multiple countries over decades. We can't prove causation the way we can with a drug trial, but the consistency and size of the effect are remarkable."
Client: "I don't have time to spend hours at the gym."
Coach: "Here's what's encouraging: even small amounts help. Studies show that just 4-5 minutes of vigorous activity per day—running to catch a bus, taking stairs quickly—is linked to 40% lower mortality. You don't have to become a gym rat to get benefits."
[CHONK: Section 2 - Strength Training: The Currency of Aging]
Strength training: The currency of aging¶
The sarcopenia crisis¶
Starting around age 30, humans lose approximately 3-8% of muscle mass per decade, with losses accelerating after age 60.[^9] This progressive loss of muscle mass and function is called sarcopenia (from Greek: sarx = flesh, penia = poverty).
Sarcopenia isn't just about looking older or feeling weaker; it's also a mortality risk factor. In a meta-analysis of 56 studies, sarcopenia approximately doubled mortality risk (HR = 2.00).[^10]
Here’s the encouraging part: muscle is highly trainable at every age, which means you can do something about this.
So what does muscle actually do for you?
- Metabolic function: Muscle is your primary glucose disposal site, so more muscle generally means better blood sugar control
- Fall prevention: Strong muscles and good balance help prevent falls, which kill more older adults than car accidents
- Functional independence: Getting out of a chair, climbing stairs, and carrying groceries all require adequate muscle
- Metabolic reserve: During illness or surgery, your body draws on muscle protein; more reserve often means better recovery
The strength training protocol¶
Based on the longevity literature and expert consensus, here's what the evidence supports:[^11] Think of this as a simple starting point, not a perfect plan you have to “get right” on day one.
- Frequency: Aim for 3-5 sessions per week, depending on schedule and recovery.
- Focus: Prioritize compound lifts that train multiple muscle groups at once.
- Principle: Use progressive overload by gradually increasing what you ask your muscles to do.
Key compound movements:
- Lower body: Squats, deadlifts, lunges, leg press (the basics for hips and legs)
- Upper body pushing: Bench press, overhead press, push-ups (pressing strength for daily life)
- Upper body pulling: Rows, pull-ups/lat pulldowns (back strength and posture support)
- Core: Planks, carries, anti-rotation exercises (trunk stability, not just “abs”)
Why compound lifts? They train multiple muscles at the same time, they look a lot like real-world movement patterns, and they’re usually more time-efficient than isolation exercises. You don't need 17 different exercises. A client who can squat, deadlift, and press has functional strength that tends to show up in everyday life.
Progressive overload: Why intensity matters¶
Client: "So if I just keep doing the same workout, I’ll keep getting stronger?"
Coach: "Your body adapts to the demands placed on it. If we lift the same weight for the same reps indefinitely, you’ll get really good at that, and then progress stalls."
Client: "Okay, so what does 'progressing' actually look like?"
Progressive overload means systematically increasing training demands over time, for example:
- Adding weight to the bar or doing more repetitions with the same weight
- Doing more sets, shortening rest periods, or improving movement quality and range of motion
This is why “showing up” to the gym matters less than actually challenging the muscles. Many people exercise for years without getting stronger because they never move beyond comfortable weights, and while starting light can feel safer (and sometimes it is), they still need a plan to gradually push past “easy.”
The dose-response for resistance training¶
A fair question is: How much is enough, and how much is too much?
A 2022 meta-analysis found that mortality risk reduction was maximal at approximately 60 minutes per week of muscle-strengthening activity, with diminishing returns at higher volumes.[^12]
In practice, that might look like 2-3 sessions of 20-30 minutes each (or 3-4 shorter sessions), as long as the priority is quality and progressive challenge.
The J-shaped curve caution: Some studies suggest very high volumes of strength training (150+ minutes/week) may not provide additional mortality benefit and could theoretically increase risk due to overtraining or injury. More isn't always better, and it's easy to end up just more tired.
Grip strength: Your longevity biomarker¶
If you want a simple, cheap, validated way to get a read on overall strength and mortality risk, look at grip strength.
Why grip strength matters:[^13][^14]
- Each 1 kg increase in grip strength is associated with 2-10% lower mortality, and the highest vs. lowest grip tertile shows 59-62% lower mortality (HR ≈ 0.38-0.41).
- It’s a strong predictor across ages (including adults 90+) and it correlates well with overall body strength.
Target: 70+ lbs (32+ kg) for longevity (as specified in the longevity protocol)
Grip strength is a proxy measure, basically a window into systemic strength. If grip is weak, other muscles are likely weak too, and if grip is improving, the client is likely getting stronger overall.
Coaching in Practice: "I Don't Want to Get Bulky"¶
What NOT to do
Client: "I want to exercise for health, but I'm worried lifting weights will make me bulky."
Coach: "I get the concern, but you really don’t need to worry about that. Just lift."
Client: "Okay... but I'm still nervous about it."
Coach: "I hear you, and you’ll probably be fine, so we can move on."
A better coaching conversation
Client: "I want to exercise for health, but I'm worried lifting weights will make me bulky."
Coach: "Yeah, I hear this a lot. Building significant muscle mass is actually very hard. It requires years of heavy training, specific nutrition, and often favorable genetics. What most people notice from strength training is feeling more capable, standing taller, and having better day-to-day energy."
Client: "But I've seen women who look really muscular..."
Coach: "Totally. That look usually comes from a deliberate plan that goes way beyond what we're talking about here. And there's another angle that's worth considering: the alternative to maintaining muscle is losing it, about 3-8% per decade after 30. That muscle loss doubles mortality risk. So it's not really 'lift weights or don't.' It's 'actively prevent muscle loss or passively accept it.'"
Client: "I guess when you put it that way..."
Coach: "How about we start with bodyweight exercises, like squats and push-ups, things you can do at home? We’ll see how you feel after a few weeks, and then decide together if we want to add anything heavier. Sound fair?"
Bone density: The skeletal connection¶
Muscle and bone health are deeply connected. The same training that builds muscle also stimulates bone:
Jump rope and plyometrics: 3x/week as recommended in the longevity protocol. Impact loading stimulates bone remodeling through mechanical stress.
Heavy resistance training: The pull of muscles on bones stimulates bone formation at attachment sites.
Why this matters: Osteoporosis (bone loss) and sarcopenia often occur together (sometimes called "osteosarcopenia"). Fractures from falls are a leading cause of death in older adults, so strength training helps address both risks at the same time. Two birds, one barbell.
Balance training: The overlooked longevity factor¶
Falls are one of the leading causes of death and disability in older adults. Each year, about one in four adults over 65 falls, and falls are the leading cause of injury-related death in this age group.[^28] The good news is that balance is trainable, and training makes a substantial difference.
The evidence for balance training:
A Cochrane review of exercise for fall prevention found:[^28]
- Any exercise reduces fall rates by approximately 23%, balance-focused and functional programs reduce falls by 24%, and multicomponent programs (balance + strength) reduce falls by 34%.
Even more striking, balance ability independently predicts mortality. In a Chinese cohort study, each additional second a person could hold a semi-tandem balance position was associated with 10% lower mortality (HR = 0.90). Those who could hold balance for 10+ seconds had 39% lower mortality than those who couldn't.[^29]
The balance training protocol:
From the longevity protocol: Balance training 2x/week, including:
- Single-leg and instability work, such as single-leg stands/deadlifts and balance boards, BOSU balls, or other unstable surfaces
- Tai Chi (or similar mind-body practices) and functional movements that challenge balance, like lunges and step-ups
Why this matters for your clients:
Falls create a vicious cycle: A fall leads to fear of falling, which leads to reduced activity, which leads to further decline in balance and strength, which increases fall risk. By the time someone has a serious fall (hip fracture, head injury), the consequences can be devastating, and hip fractures in older adults carry a one-year mortality rate of 20-30%.
For clients over 50, balance work isn't optional; it's essential preventive medicine. Two 15-20 minute sessions per week can dramatically reduce fall risk and help preserve independence. If that feels like one more thing to pile on, start small and build. Small doses count.
| For DIY Learners |
|---|
| Applying this to yourself: Try this quick balance test right now: Stand on one leg, then close your eyes, and time how long you can hold it. If you can't reach 10 seconds, that's a signal to add balance work to your routine. Start with single-leg stands during your daily routine (while brushing teeth, waiting for coffee, or during TV commercials), and build from there. |
Coaching in Practice: "Balance Training? That's for Old People"¶
What NOT to do
Client: "Balance training? Come on, that's for old people in rehab, and I'm fine, really."
Coach: "Well, you're wrong, and everyone needs balance training."
Client: "Okay..."
A better coaching conversation
Client: "Balance training? Come on, that's for old people in rehab, and I'm fine, really."
Coach: "I get why it sounds that way. Elite athletes do balance work, and it improves performance and helps prevent injury; the same principle applies to everyone. Better balance usually means better movement quality, fewer falls, and more independence as you age."
Client: "But I don't fall."
Coach: "Totally. Think of it like insurance. You don't get car insurance because you're a bad driver, you get it because accidents happen, and falls become increasingly dangerous with age. Hip fractures in older adults have a 20-30% mortality rate within a year, so balance training is basically insurance against that."
Client: "What would I even do?"
Coach: "We can keep it simple: Stand on one foot while brushing your teeth, do heel-to-toe walking down the hallway, or try single-leg stands while your coffee brews. Two 15-minute sessions a week can make a real difference. Want to try standing on one foot right now?"
[CHONK: Section 3 - Zone 2 Cardio: Building Mitochondrial Efficiency]
Zone 2 cardio: Building mitochondrial efficiency¶
What is Zone 2?¶
Zone 2 refers to a specific intensity of aerobic exercise: the highest intensity where your body can still primarily use fat for fuel while keeping lactate levels stable. In more technical terms, that means exercise at or just below the first ventilatory threshold (VT1). It sounds a little science-y, but the feel is usually easier to coach than the physiology.
In practical terms, Zone 2 feels like:
- You can hold a conversation, but it takes a little effort
- You're breathing noticeably harder than at rest, yet you could sustain this pace for an hour or more
- On a 1-10 scale, it's about a 4-5
Why this specific intensity matters:
As we discussed in Chapter 1.2 (Biology of Aging), mitochondrial dysfunction is one of the hallmarks of aging. Mitochondria are the "power plants" of your cells, producing the energy (ATP) that runs every biological process, from muscle contraction to brain function. They matter a lot.
Zone 2 training is a particularly good way to drive mitochondrial adaptations:[^15]
- Increases mitochondrial density and efficiency
- Improves fat oxidation and the ability to use oxygen at the cellular level
- Builds the aerobic "base" that supports other activity, including higher-intensity work
The Zone 2 protocol¶
Duration: 150-300 minutes per week (as recommended in the longevity protocol)
This typically translates to either:
- 30-60 minutes, 3-5 times per week
- Or longer sessions fewer times per week
How to determine your Zone 2:
Zone 2 varies a lot from person to person, which is why generic heart rate formulas (like "180 minus age") often miss the mark. Here are a few practical ways to find it:[^16] If the numbers and thresholds start to blur together, that’s normal. You don’t need perfect precision to help clients get real results.
1. The Talk Test (most practical)
The Talk Test has been validated as a reasonable proxy for VT1.[^17] Here’s the boundary:
- Below Zone 2: Can speak easily and sing
- Zone 2: Can speak in full sentences, but it requires some effort; singing would be difficult
- Above Zone 2: Can only speak in short phrases or single words
2. Heart Rate Method
For many people, VT1 corresponds to approximately 60-70% of maximum heart rate, or about 40% of heart rate reserve. Fitness level matters, though, because people who are fitter often reach VT1 at a higher percentage of their max.
The basic formula: Max HR ≈ 220 - age, so for a 50-year-old, estimated max HR is 170 (220 - 50), and Zone 2 would be roughly 102-119 bpm (60-70% of 170).
Heart Rate Reserve (HRR) method (more accurate):
1. Calculate max HR (220 - age), and note your resting HR.
2. Subtract resting HR from max HR to get HRR (your usable heart rate range for exercise).
3. Multiply HRR by your target percentage (about 40% for Zone 2) to get your training “slice” of that reserve.
4. Add your resting HR back to estimate your Zone 2 heart rate.
Example: For a 50-year-old with a resting HR of 60, max HR = 170 and HRR = 110 (170 - 60), so the Zone 2 target is (110 × 0.40) + 60 = 104 bpm.
Think of these as starting points, not truth-with-a-capital-T. Individual variation is substantial, which is exactly why the Talk Test remains the go-to option for most clients. In practice, most clients don’t need to obsess over the exact bpm.
3. Lactate Testing (most accurate)
Laboratory testing with blood lactate measurements can precisely identify your thresholds. It’s the gold standard, but it requires access to testing facilities and a client who wants to do it.
Coaching in Practice: Teaching the Talk Test¶
What NOT to do¶
Client: “How do I know I’m in Zone 2?”
Coach: “Zone 2 is the highest intensity where you’re still primarily oxidizing fat while keeping lactate stable, which is basically around VT1.”
Client: “VT1?”
Coach: “First ventilatory threshold. Your heart rate should be about 60-70% of max, unless your heart rate reserve changes it, and then we’d calculate that with the Karvonen formula.”
Client: “Okay… so what am I supposed to do on the bike?”
Coach: “Ideally, we’d confirm your threshold with lactate testing.”
Better: Teach the Talk Test (dialogue)¶
Client: “How do I know I’m in Zone 2? I don’t want to guess.”
Coach: “Totally fair, and the Talk Test is a simple way to get close. While you’re moving, try saying a full sentence out loud.”
Client: “Like… ‘I’m doing my workout and I feel okay’?”
Coach: “Exactly. If you can say that in a full sentence but it takes a little effort, you’re probably in Zone 2. If you can sing, you’re likely below it. If you can only get out a few words at a time, you’ve drifted above it.”
Client: “So the goal is ‘talking is possible, but not effortless.’”
Coach: “You’ve got it. And it might take a couple sessions to dial in, especially if you’re used to going harder.”
Zone 2 isn't magic, but it's effective¶
A little humility is appropriate here. Zone 2 is popular in longevity circles, but the evidence doesn’t support the claim that it’s uniquely superior to other intensities.
A 2025 Sports Medicine review concluded that Zone 2 is not superior to higher-intensity training for mitochondrial signaling or VO2 max improvements.[^18] In fact, higher-intensity exercise creates greater energetic stress and may lead to stronger adaptations.
If you’re thinking, “Wait, so why am I doing Zone 2 then?”, you’re not alone. The point isn’t that Zone 2 is the answer; it’s that it’s a workable piece of a complete plan.
So why recommend Zone 2?
Several reasons:
1. Sustainability: It’s a pace most people can repeat week after week without burning out
2. Low injury risk: It’s generally easier on joints and connective tissue than harder efforts
3. Time efficiency for busy people: It can be done often with minimal recovery cost
4. Builds foundation: It creates an aerobic base that supports higher-intensity work
5. Can be combined with other activities: Walking meetings, commuting by bike, and social activities can all count
The ideal approach includes both Zone 2 work and higher-intensity training, which we'll cover in the next section.
What about higher-intensity cardio?¶
The intensity vs. volume debate continues in exercise science, and the data keep pointing to intensity as an important piece of the puzzle. A 2025 NHANES accelerometer study found that intensity was a stronger predictor of mortality than volume: moving from the 25th to 50th percentile of intensity reduced mortality risk by 37%, compared to 14% for the same shift in volume.[^19]
This doesn’t mean Zone 2 is worthless. It means a complete approach includes both:
- Zone 2 (150-300 min/week): Builds aerobic base, mitochondrial density
- Higher intensity (discussed next section): Maximizes VO2 max, cardiovascular reserve
[CHONK: Section 4 - VO2 Max Training: The Vital Sign]
VO2 max training: The vital sign¶
Why VO2 max predicts mortality¶
VO2 max is the maximum amount of oxygen your body can use during intense exercise, and among fitness and health biomarkers, it’s arguably the single strongest predictor of all-cause mortality.[^20] That’s a big statement, but the data backs it up.
Recall from Chapter 1.4 (Assessment and Biomarkers) that each 1-MET increase in cardiorespiratory fitness associates with 11-17% lower mortality. In the Cleveland Clinic study, elite fitness (top 2-3%) showed 5-fold lower mortality compared to the least fit quintile.[^21]
The practical takeaway: improving your aerobic fitness is one of the most reliable ways to stack the odds in your favor.
Target: 35+ mL/kg/min for longevity protection (per the longevity protocol)
For reference:
- Average untrained adult: ~35 mL/kg/min (women), ~42 mL/kg/min (men)
- Well-trained recreational athletes: 45-55 mL/kg/min
- Elite endurance athletes: 60-80+ mL/kg/min
- Values decline with age (~1% per year without training)
The good news is that VO2 max is trainable. With proper training, improvements of 15-20% are common, and some studies show gains of 6-13% in just 8 weeks with high-intensity protocols.[^22] Not everyone responds the same way, but most people can move the needle.
The Norwegian 4x4 protocol¶
For clients ready for VO2 max training (meaning they already have their fundamentals established), the Norwegian 4x4 protocol is the most commonly recommended approach:[^23]
The workout:
- 4 intervals of 4 minutes each
- Work at 90-95% of maximum heart rate
- 3 minutes active recovery between intervals (walking or easy jogging)
- Frequency: 1x per week
Why it works: Four minutes is long enough at high intensity to accumulate significant time above 90% of VO2 max, which is the threshold needed to stimulate maximum adaptation. Shorter sprints often don’t allow heart rate and oxygen consumption to reach maximal levels.
A 2023 study found: 8 weeks of the 4x4 protocol increased VO2 max by ~6.5% compared to ~3.3% with sprint interval training.[^22]
This is advanced optimization¶
Key context: VO2 max training belongs in the “advanced optimization” category, not the fundamentals.
The hierarchy matters:
1. Any movement (walking, basic activity)
2. Strength training (prevents sarcopenia, builds metabolic machinery)
3. Zone 2 cardio (builds aerobic base, sustainable long-term)
4. VO2 max training (maximizes cardiovascular ceiling)
So if a client isn’t exercising at all, they shouldn’t start with 4x4 intervals. And if they’re sleeping 5 hours a night, adding high-intensity training to an already-stressed system usually makes things worse, not better. Get the fundamentals right first, then optimize. You don’t have to do everything at once.
Safety considerations¶
High-intensity training carries some risk, particularly for:
- Previously sedentary individuals
- Those with known or unknown cardiovascular disease
- Clients over 50 who haven't exercised regularly
Staying in your scope here protects your client and protects you. And it builds trust.
Within your scope, you can:
- Encourage clients to get medical clearance before starting intense exercise
- Suggest they work with a qualified fitness professional for program design
- Help them recognize warning signs (chest pain, unusual shortness of breath, dizziness)
- Support gradual progression from lower intensities
Outside your scope:
- Prescribing specific VO2 max protocols
- Determining whether a client is medically cleared for intense exercise
- Designing periodized training programs
Coaching in Practice: "What's VO2 Max and Why Should I Care?"¶
Client: "My friend keeps talking about his VO2 max. What even is that?"
Coach: "VO2 max measures how efficiently your body uses oxygen. Think of it as your cardiovascular system’s horsepower. Research shows it’s one of the strongest predictors of how long you’ll live, even stronger than cholesterol levels or blood pressure."
Client: "Is mine probably bad?"
Coach: "Hard to say without testing, but here’s the good news: it’s trainable. Unlike some genetic factors you can’t change, you can meaningfully improve your VO2 max with the right kind of exercise, and even modest improvements translate to measurable reductions in mortality risk."
Programming for life: Practical implementation¶
Combining modalities¶
The evidence is clear: combined training beats single-modality approaches. But what does that look like in real life, with real schedules? (Because that’s where things usually get sticky.)
Here’s a simple structure you can use to talk through exercise programming with clients. It’s not a prescription, just a conversation guide.
Weekly targets (from the longevity protocol):
- Strength training: 3-5 sessions
- Zone 2 cardio: 150-300 minutes total
- VO2 max training: 1 session (for those ready)
- Mobility: 10-15 minutes daily
- Balance training: 2 sessions (especially important for older clients)
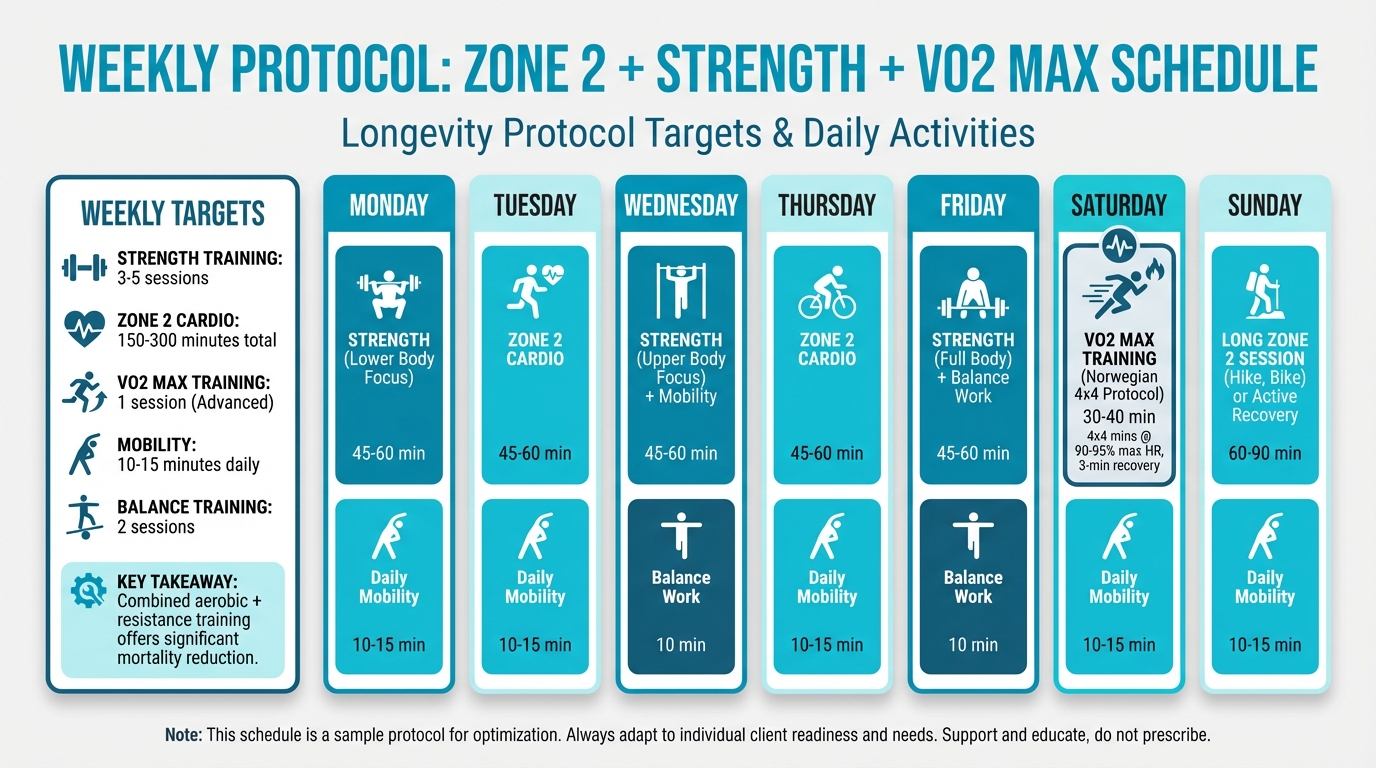
Figure: Zone 2 + Strength + VO2 max weekly schedule
Sample weekly schedules¶
Important caveat: These are conversation guides, not prescriptions. Exercise programming should be done by qualified fitness professionals. Your role is to support clients in finding sustainable approaches, then help connect them with the right resources when needed. (It’s okay to be the guide, not the person “writing the program.”)
The "Minimum Effective Dose" Week (for time-constrained clients):
| Day | Activity | Duration |
|---|---|---|
| Monday | Strength training (full body) | 30-45 min |
| Tuesday | Zone 2 cardio (walk, bike, swim) | 30-45 min |
| Wednesday | Rest or light movement | . |
| Thursday | Strength training (full body) | 30-45 min |
| Friday | Zone 2 cardio | 30-45 min |
| Saturday | Longer Zone 2 session OR active hobby | 45-90 min |
| Sunday | Rest or mobility work | 15-30 min |
Total: ~3-4 hours/week of structured exercise
The "Optimal Dose" Week (for clients with more time and established fitness):
| Day | Activity | Duration |
|---|---|---|
| Monday | Strength (lower body focus) | 45-60 min |
| Tuesday | Zone 2 cardio | 45-60 min |
| Wednesday | Strength (upper body focus) + mobility | 45-60 min |
| Thursday | Zone 2 cardio | 45-60 min |
| Friday | Strength (full body) + balance work | 45-60 min |
| Saturday | VO2 max training (4x4 protocol) | 30-40 min |
| Sunday | Long Zone 2 session (hike, bike) or active recovery | 60-90 min |
Total: ~6-8 hours/week of structured exercise
Gender considerations¶
The longevity protocol notes some female-specific considerations worth understanding:
Menstrual cycle and training:
- Follicular phase (day 1 through ovulation): Generally can handle higher intensity and volume; estrogen supports recovery
- Luteal phase (post-ovulation through menstruation): Some women benefit from slightly reduced intensity; progesterone can affect perceived exertion
The key principle: Consistency matters more than perfection. (If tracking the cycle feels like “one more thing,” you’re not alone.)
Research on menstrual cycle and performance is still evolving. Some studies show performance variations across the cycle; others show no significant difference. The practical guidance:[^24]
- Don't downregulate training without data: Many women unnecessarily reduce training during their period based on assumptions rather than their actual response
- Track and learn: If a client notices consistent patterns, they can adjust accordingly
- Avoid perfectionism: The science isn't settled enough to warrant complex periodization based on cycle phase
Women and strength training: Women may need slightly different approaches:
- Pay attention to iron status (menstrual blood loss affects iron)
- Ensure adequate protein (many women undereat protein)
- Embrace heavy weights (fears of "bulking" are usually unfounded)
- Don't over-rely on cardio at the expense of strength work
Age considerations¶
Exercise benefits appear at every age, including for those who start later in life.
Key research findings:
- Meeting physical activity guidelines associated with ~22% lower mortality regardless of age[^25]
- Benefits don't diminish with older age, if anything, relative risk reductions may be larger
- Initiating exercise later in life can still improve outcomes when maintained long-term
For older clients:
- Balance training becomes increasingly important (fall prevention)
- Recovery may take longer: adequate rest between sessions
- Joint-friendly modifications may be needed (swimming, cycling vs. running)
- Strength training is arguably more important, not less, as sarcopenia accelerates
The "it's too late" myth: Help clients understand that starting at 50, 60, or even 70 still provides meaningful benefits. The alternative, continued inactivity, has clear costs. (If they’re discouraged, that’s a human response, not a character flaw.)
Finding the minimum effective dose¶
Not every client will train like an athlete, and that’s okay. The goal is sustainable movement that continues for decades, not maximum-intensity training that burns clients out.
Questions to explore with clients:
- What's the minimum they could commit to consistently?
- What forms of movement do they actually enjoy?
- What barriers exist, and which are negotiable?
- What does success look like for their life, not someone else's?
For a busy executive who travels constantly, maintaining strength training 2x/week and walking daily might be their realistic optimum. For a retiree with ample time, a more complete approach becomes feasible.
The research supports this flexibility: Benefits appear well below "optimal" levels. A 2022 study found that even "weekend warrior" patterns (concentrating activity in 1-2 days) showed comparable mortality reductions to more evenly distributed exercise, provided total volume was similar.[^26]
[CHONK: Section 6 - Deep Health Integration]
Deep Health integration¶
Exercise touches every dimension of Deep Health, so when you're working with clients on movement, it helps to zoom out and connect the workouts to the bigger picture of their wellbeing. This means exercise can help in more ways than most people realize.
Physical health¶
This one’s pretty straightforward: exercise directly impacts:
- Cardiovascular function: Heart muscle strength, blood vessel health, blood pressure
- Metabolic health: Insulin sensitivity, glucose disposal, body composition
- Musculoskeletal health: Muscle mass, bone density, joint function
- Immune function: Moderate exercise supports immune health (though excessive training can suppress it)
If clients see exercise only as a weight-management tool, help them notice the broader physical benefits, many of which can happen even if their weight doesn’t change. That can feel surprisingly validating for people who’ve been “doing everything right” and not seeing the scale move.
Mental/cognitive health¶
Exercise is a nootropic, meaning it can support brain function. The mechanisms include:[^27]
- BDNF release: Brain-derived neurotrophic factor, sometimes called "Miracle-Gro for the brain," increases with exercise
- Neurogenesis: New brain cell formation, particularly in the hippocampus (memory center)
- Cerebral blood flow: More oxygen and nutrients delivered to brain tissue
- Reduced inflammation: Chronic inflammation impairs cognitive function; exercise is anti-inflammatory
The longevity protocol specifically notes: "Exercise as a nootropic: vigorous exercise such as VO2 max training."
Dual-task activities, those requiring simultaneous physical and cognitive processing (dance, martial arts, tennis, racket sports), may build cognitive reserve more effectively than repetitive exercise because they engage multiple neural networks.
Emotional health¶
Exercise rivals medication for treating mild-to-moderate depression and anxiety. Research shows that a single bout can improve mood in the moment, while regular exercise reduces depression risk over time. These effects also appear independent of fitness improvements, so it’s not just about “getting in shape.”
For clients who are struggling emotionally, exercise can be part of a whole-person approach. It’s not a replacement for mental health treatment when that’s needed, but it can be a powerful complementary tool.
Social/relational health¶
Movement can also be a connection point:
- Group fitness classes: Built-in community
- Sports and recreational activities: Shared goals and experiences
- Walking meetings: Combining productivity with movement
- Family activities: Hiking, biking, playing together
For socially isolated clients, exercise groups can meet two needs at the same time, and having workout partners often supports consistency through simple accountability.
Environmental health¶
The environment matters too. Explore what exercise looks like in the client’s real life:
- Outdoor activity: Exposure to nature adds benefits beyond the exercise itself ("green exercise")
- Air quality: Urban outdoor exercise during high-pollution periods may have trade-offs
- Access: Does the client have safe places to walk? Affordable gym access? Home equipment?
- Seasonal considerations: How will their routine adapt to weather changes?
Environmental barriers are often the unspoken reasons clients don’t exercise. A client without safe walking routes or gym access faces different challenges than someone with a home gym and suburban trails, and it helps to name that without judgment. It’s also normal for people to blame “motivation” when the real issue is logistics.
Existential/purposeful health¶
One of the most powerful questions you can ask is: What do you want 80-year-old you to be able to do?
This connects exercise to meaning and purpose:
- Playing on the floor with grandchildren
- Traveling independently
- Maintaining hobbies (golf, gardening, hiking)
- Not being a burden on family members
- Continuing to contribute to community
Exercise for longevity isn’t about vanity, or even disease prevention in the abstract. It’s about preserving the functional capacity to live a meaningful life, so help clients connect their movement habits to their deeper values and long-term vision.
Coaching in Practice: The "80-Year-Old You" Conversation¶
What NOT to do
Client: "I know I should exercise, but I just can't seem to stick with it. I don't really care about losing weight."
Coach: "You still need to do it. Just focus on the scale, cut your calories, and push yourself harder."
Client: "That’s not really what I’m looking for."
Coach: "Well, if you want results, you have to want weight loss."
A better approach
Client: "I know I should exercise, but I just can't seem to stick with it. I don't really care about losing weight."
Coach: "That makes sense, and if weight loss isn’t motivating, it’s hard to stay consistent. Would you be open to trying a different angle?"
Client: "Sure, I'm open to that."
Coach: "Close your eyes for a second and imagine your ideal 80-year-old self. What do they look like, and what are they able to do?"
Client: "I don’t know... maybe travel, play with grandkids, and not be a burden on anyone."
Coach: "Got it. Want to hear how exercise connects to that?"
Client: "Yeah, I'd like that."
Coach: "Things like muscle loss, lower cardiovascular capacity, poorer balance that can lead to falls, and reduced mobility are often what get in the way of that kind of independence."
Client: "Yeah, I've seen that happen to people."
Coach: "Exactly. The exercise you do now (or don’t do) is either building or eroding the physical capabilities of that future person. Strength training, cardio, and balance work are basically investments in your 80-year-old self’s independence."
Client: "When you put it that way, it feels more important."
Coach: "If you imagine you’re looking back from 80, what would you regret not having done?"
[CHONK: Key Takeaways and Summary]
Key takeaways¶
-
Exercise is the #1 longevity intervention: Combined aerobic and resistance training reduces mortality by approximately 40%, and no supplement, medication, or biohack comes close to that effect.
-
Cardiorespiratory fitness predicts survival: Each 1-MET increase in VO2 max associates with 11-17% lower mortality, so a practical target is 35+ mL/kg/min.
-
Strength training prevents sarcopenia: Sarcopenia doubles mortality risk, which is why 3-5 sessions/week of compound lifts with progressive overload can be so protective. Grip strength (target: 70+ lbs) is a useful biomarker too.
-
Zone 2 builds the aerobic foundation: 150-300 minutes/week of cardio where you can hold a conversation builds mitochondrial efficiency, and the Talk Test is a straightforward way to find your zone. (Spoiler: you don’t need fancy gear.)
-
VO2 max training is advanced optimization: The Norwegian 4x4 protocol (1x/week) maximizes cardiovascular ceiling, but it’s best reserved for clients who already have the fundamentals established.
-
Combined training beats either modality alone: Both cardio and strength matter, so the question isn’t either/or. It’s both/and. (Simple, not easy.)
-
Benefits occur at any age: It’s never too late to start, and even small amounts of activity dramatically reduce mortality compared to complete inactivity, even if you or your client is starting from zero. (Everyone starts somewhere.)
-
Your role is support, not prescription: You can educate clients on the evidence, help them connect exercise to their values, facilitate behavior change, and connect them with fitness professionals for program design.
What not to do: write detailed training programs if that’s outside your scope.
Better:
Client: “Can you build me a workout plan?”
Coach: “I can help you choose the right focus and build the habit, and then I’ll connect you with a qualified trainer for the programming details.”
[CHONK: Study guide questions]
Study Guide Questions¶
Here are some questions that can help you think through the material and prepare for the chapter exam. They're optional, but we recommend you try answering at least a few as part of your active learning process.
-
What is the approximate mortality reduction associated with combined aerobic and resistance training compared to inactivity?
-
Why is VO2 max considered one of the strongest predictors of longevity? What's the target value mentioned in the protocol?
-
Explain what sarcopenia is and why it matters for longevity.
-
Describe how to use the Talk Test to determine Zone 2 intensity.
-
What is the Norwegian 4x4 protocol and who is it appropriate for?
-
As a health coach, what is within your scope regarding exercise, and what requires referral to other professionals?
Self-reflection questions:
-
Audit your own exercise habits: How many minutes of Zone 2 cardio do you get weekly? How often do you strength train? What's the biggest gap between your current habits and the longevity protocol?
-
Do you know your VO2 max? If not, what's one way you could estimate or measure it this month?
Further Reading¶
If you'd like more detail, these supplemental articles explore key topics from this chapter.
- Zone 2 Training Science covers lactate thresholds and mitochondrial biogenesis.
- Strength Training Programming goes beyond the basics for longevity.
References¶
-
Saeidifard F, Medina-Inojosa JR, West CP, Olson TP, Somers VK, Bonikowske AR, et al. The association of resistance training with mortality: A systematic review and meta-analysis. European Journal of Preventive Cardiology. 2019;26(15):1647-1665. doi:10.1177/2047487319850718
-
Momma H, Kawakami R, Honda T, Sawada SS. Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: a systematic review and meta-analysis of cohort studies. British Journal of Sports Medicine. 2022;56(13):755-763. doi:10.1136/bjsports-2021-105061
-
Zhao M, Veeranki SP, Magnussen CG, Xi B. Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study. BMJ. 2020:m2031. doi:10.1136/bmj.m2031
-
Yu R, Duncombe SL, Nemoto Y, Araujo RH, Chung H, Mielke GI. Physical activity trajectories and accumulation over adulthood and their associations with all-cause and cause-specific mortality: a systematic review and meta-analysis. British Journal of Sports Medicine. 2025;59(17):1228-1241. doi:10.1136/bjsports-2024-109122
-
Lang JJ, Prince SA, Merucci K, Cadenas-Sanchez C, Chaput J, Fraser BJ, et al. Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies. British Journal of Sports Medicine. 2024;58(10):556-566. doi:10.1136/bjsports-2023-107849
-
Stamatakis E, Ahmadi MN, Gill JMR, Thøgersen-Ntoumani C, Gibala MJ, Doherty A, et al. Association of wearable device-measured vigorous intermittent lifestyle physical activity with mortality. Nature Medicine. 2022;28(12):2521-2529. doi:10.1038/s41591-022-02100-x
-
Bahls M, Kavousi M, Bakker EA, Kränkel N, Baurecht H, Timmermans EJ, et al. Physical activity and mortality: towards healthspan-oriented metrics and outcomes. A Scientific Statement from the European Association of Preventive Cardiology (EAPC) of the ESC. European Journal of Preventive Cardiology. 2025. doi:10.1093/eurjpc/zwaf578
-
Coenen P, Huysmans MA, Holtermann A, Troiano RP, Mork PJ, Krokstad S, et al. Associations of occupational and leisure-time physical activity with all-cause mortality: an individual participant data meta-analysis. British Journal of Sports Medicine. 2024;58(24):1527-1538. doi:10.1136/bjsports-2024-108117
-
Huang Y, Gao L, Xie X, et al. Sarcopenia is associated with mortality in adults: a systematic review and meta-analysis. Gerontology; 2021. https://pubmed.ncbi.nlm.nih.gov/34315158/
-
Shailendra P, Baldock KL, Li LK, Bennie JA, Boyle T. Resistance Training and Mortality Risk: A Systematic Review and Meta-Analysis. American Journal of Preventive Medicine. 2022;63(2):277-285. doi:10.1016/j.amepre.2022.03.020
-
López-Bueno R, Andersen LL, Calatayud J, Casaña J, Grabovac I, Oberndorfer M, et al. Associations of handgrip strength with all-cause and cancer mortality in older adults: a prospective cohort study in 28 countries. Age and Ageing. 2022;51(5). doi:10.1093/ageing/afac117
-
Andersen LL, López‐Bueno R, Núñez‐Cortés R, Cadore EL, Polo‐López A, Calatayud J. Association of Muscle Strength With All‐Cause Mortality in the Oldest Old: Prospective Cohort Study From 28 Countries. Journal of Cachexia, Sarcopenia and Muscle. 2024;15(6):2756-2764. doi:10.1002/jcsm.13619
-
Jun L, Knight E, Broderick TL, Al-Nakkash L, Tobin B, Geetha T, et al. Moderate-Intensity Exercise Enhances Mitochondrial Biogenesis Markers in the Skeletal Muscle of a Mouse Model Affected by Diet-Induced Obesity. Nutrients. 2024;16(12):1836. doi:10.3390/nu16121836
-
Milani JGPO, Milani M, Cipriano GFB, Hansen D, Cipriano Junior G. Exercise intensity domains determined by heart rate at the ventilatory thresholds in patients with cardiovascular disease: new insights and comparisons to cardiovascular rehabilitation prescription recommendations. BMJ Open Sport & Exercise Medicine. 2023;9(3):e001601. doi:10.1136/bmjsem-2023-001601
-
Kwon Y, Kang KW, Chang JS. The talk test as a useful tool to monitor aerobic exercise intensity in healthy population. Journal of Exercise Rehabilitation. 2023;19(3):163-169. doi:10.12965/jer.2346170.085
-
Storoschuk KL, Moran-MacDonald A, Gibala MJ, Gurd BJ. Much Ado About Zone 2: A Narrative Review Assessing the Efficacy of Zone 2 Training for Improving Mitochondrial Capacity and Cardiorespiratory Fitness in the General Population. Sports Medicine. 2025;55(7):1611-1624. doi:10.1007/s40279-025-02261-y
-
Schwendinger F, Infanger D, Lichtenstein E, Hinrichs T, Knaier R, Rowlands AV, et al. Intensity or volume: the role of physical activity in longevity. European Journal of Preventive Cardiology. 2024;32(1):10-19. doi:10.1093/eurjpc/zwae295
-
Ding J, et al. Comparison of objectively measured and estimated cardiorespiratory fitness to predict all-cause and cardiovascular disease mortality in adults. J Sport Health Sci; 2025. https://pubmed.ncbi.nlm.nih.gov/39271056/
-
Mandsager K, Harb S, Cremer P, Phelan D, Nissen SE, Jaber W. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Network Open. 2018;1(6):e183605. doi:10.1001/jamanetworkopen.2018.3605
-
Hov H, Wang E, Lim YR, Trane G, Hemmingsen M, Hoff J, et al. Aerobic
high‐intensity intervals are superior to improve V̇O2max compared with sprint intervals inwell‐trained men. Scandinavian Journal of Medicine & Science in Sports. 2022;33(2):146-159. doi:10.1111/sms.14251 -
Martinez-Gomez D, Luo M, Huang Y, Rodríguez-Artalejo F, Ekelund U, Sotos-Prieto M, et al. Physical Activity and All-Cause Mortality by Age in 4 Multinational Megacohorts. JAMA Network Open. 2024;7(11):e2446802. doi:10.1001/jamanetworkopen.2024.46802
-
Ren R, Wang W, Liu Q, Ye X, Xi L, Zhang R, et al. Dual Cohort Insights Into Accelerometer‐Derived Weekend Warrior Physical Activity and Its Impact on Mortality. Journal of the American Heart Association. 2025;14(11). doi:10.1161/jaha.124.039852
-
Gillespie SH, et al. Exercise for preventing falls in older people living in the community: an abridged Cochrane review. Br J Sports Med; 2019. https://pubmed.ncbi.nlm.nih.gov/31792067/
-
Cao C, Cade WT, Li S, McMillan J, Friedenreich C, Yang L. Association of Balance Function With All-Cause and Cause-Specific Mortality Among US Adults. JAMA Otolaryngology–Head & Neck Surgery. 2021;147(5):460. doi:10.1001/jamaoto.2021.0057
-
U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd edition. 2018. https://health.gov/our-work/nutrition-physical-activity/physical-activity-guidelines/current-guidelines