Unit 3: Advanced Topics & Disease Prevention¶
Chapter 3.17: Metabolic Disease & Inflammation¶
[CHONK: 1-minute summary]
What you'll learn in this chapter:
- How insulin resistance develops and progresses toward Type 2 Diabetes
- The concept of "inflammaging": chronic low-grade inflammation that accelerates aging
- What inflammation biomarkers like hsCRP measure (and what coaches can/cannot do with this information)
- Evidence that metabolic disease can be reversed through lifestyle changes
- How to support clients with metabolic risk factors within your scope of practice
- When metabolic concerns require medical referral
The big idea: Metabolic disease (particularly insulin resistance and Type 2 Diabetes) and chronic inflammation aren't separate problems. They're deeply interconnected, and both accelerate aging. The hopeful news: research shows these conditions can often be improved or even reversed through lifestyle changes. But here's where it gets tricky for coaches: metabolic disease sits squarely at the intersection of coaching and medicine. Understanding the biology helps you support clients effectively, and understanding your scope boundaries keeps them safe. This chapter gives you both.
What this means for your clients: Many of your clients either have metabolic concerns already (perhaps their doctor mentioned "prediabetes") or they're at risk. With this chapter, you'll understand what's happening in their bodies, know the evidence for improvement, and be able to support their lifestyle changes while staying firmly within your scope, always working alongside, never in place of, their medical team.
Introduction¶
In Chapter 2.8, we covered metabolic health strategies that benefit everyone: blood sugar management, meal composition, and time-restricted eating. That chapter was about optimization for healthy people.
This chapter goes deeper, and it gets a bit darker.
We're talking about what happens when metabolic health breaks down: insulin resistance develops, Type 2 Diabetes emerges, and chronic inflammation quietly accelerates aging from the inside. These are disease processes, not just optimization targets.
Why does this matter for you as a longevity coach?
Because metabolic dysfunction is one of the biggest threats to healthspan and lifespan. Metabolic syndrome (that cluster of high blood sugar, high blood pressure, excess abdominal fat, and abnormal cholesterol) affects roughly one in three American adults. Having it increases the risk of dying from heart disease by 44 percent and from diabetes by more than five-fold.
And chronic inflammation? Researchers call it "inflammaging," a persistent, low-grade inflammatory state that accelerates aging and contributes to virtually every age-related disease.
If those statistics feel alarming, that's a reasonable response. They should get your attention. But here's the key point: you don't need to memorize the percentages. What matters is understanding that metabolic health and inflammation are major levers, and they're levers you and your clients can actually move.
But the hopeful part is that both metabolic disease and chronic inflammation respond to lifestyle changes. The DiRECT trial showed that 46 percent of people with Type 2 Diabetes achieved remission at one year through an intensive diet program.24 Regular exercise reduces inflammatory markers significantly.48
As a coach, you won't diagnose these conditions, interpret labs, or prescribe treatments. Your medical colleagues do that. But you will help clients implement the lifestyle changes their doctors recommend. You'll support behavior change, build sustainable habits, and help clients navigate the emotional complexity of living with metabolic concerns.
What not to do
Client: "My doctor said I'm prediabetic. What should I do?"
Coach: "You probably need medication, and you should start cutting carbs right away."
A better approach
Client: "My doctor said I'm prediabetic. What should I do?"
Coach: "Thanks for sharing that, and I can hear this is weighing on you. I can't diagnose or prescribe, but I can help you follow your clinician's plan and build the day-to-day habits that make it work. What did your doctor recommend, and what feels hardest to put into practice right now?"
That's why you need to understand this biology. Not to practice medicine, but to be an effective partner in care.
First up: a clear picture of what we're dealing with.
[CHONK: Metabolic Health: The Foundation]
Metabolic Health: The Foundation¶
To talk about metabolic disease, we first need a clear, practical definition of metabolic health.
What Is Metabolic Health?¶
At its simplest, metabolic health is about how well your body processes and uses energy from food.
In plain terms, when you eat, your body breaks down carbohydrates into glucose (blood sugar), which your cells can use for fuel. Insulin, a hormone made by your pancreas, works like a key that opens the "door" to your cells so glucose can get in. (Not a perfect metaphor, but it gets the idea across.)
In a metabolically healthy person, this system tends to run smoothly:
- Blood sugar rises after eating, then returns to baseline
- Insulin does its job efficiently (cells respond well to the "key")
- Cells readily absorb glucose for energy
- The body can switch easily between burning glucose and burning fat
That last point, the ability to switch fuel sources, is called metabolic flexibility, and you covered it in Chapter 2.8. Put simply, healthy metabolic function means your body can adapt to different energy demands without getting stuck in one mode.
The Five Markers of Metabolic Syndrome¶
Doctors identify metabolic syndrome when someone has three or more of five specific conditions:20
- Large waist circumference: More than 40 inches for men, more than 35 inches for women (these thresholds vary by ethnicity)
- High triglycerides: 150 mg/dL or higher
- Low HDL cholesterol: Less than 40 mg/dL for men, less than 50 mg/dL for women
- High blood pressure: 130/85 mmHg or higher
- High fasting blood sugar: 100 mg/dL or higher
Important scope note: These are medical diagnostic criteria, which means you cannot diagnose metabolic syndrome (only a licensed healthcare provider can). Still, knowing these markers helps you understand what your clients are facing when their doctor flags metabolic concerns.
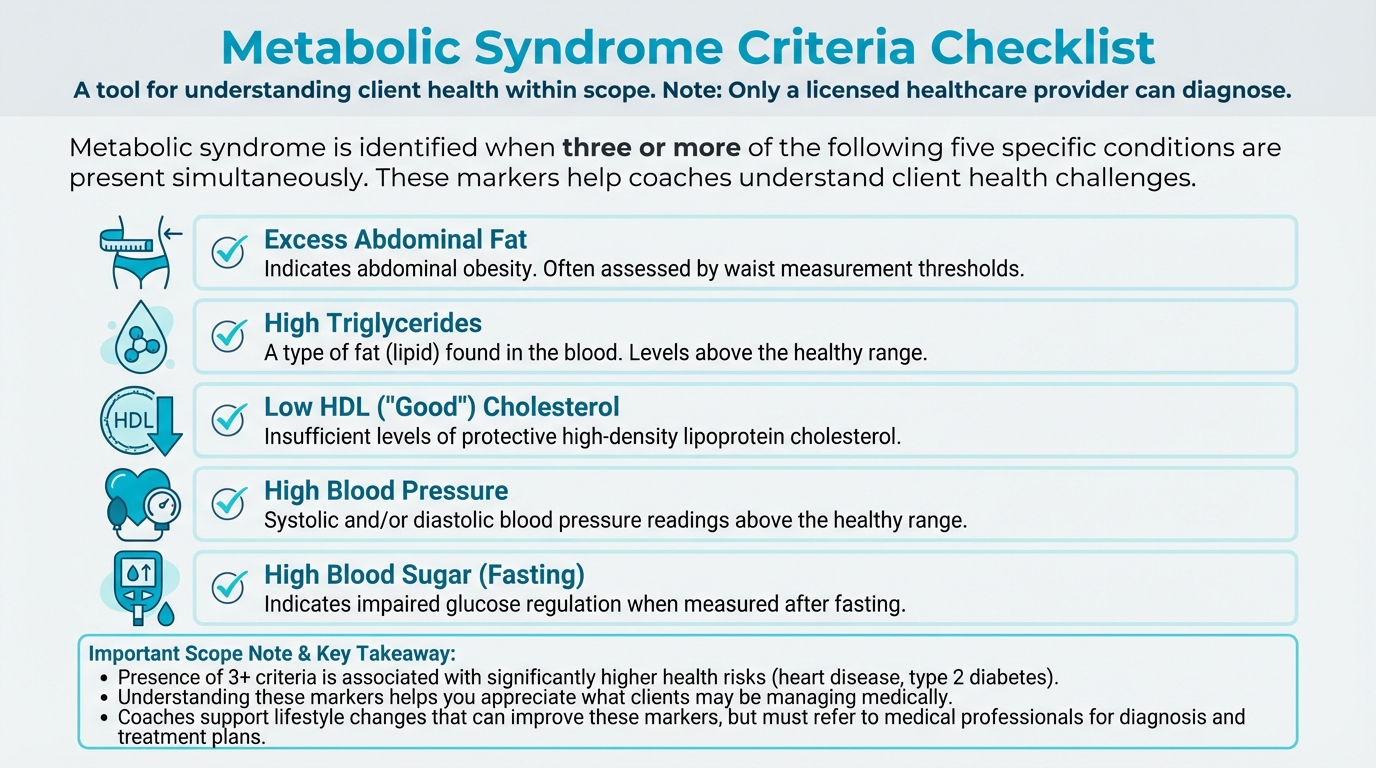
Figure: 5 criteria visual
The Metabolic Health Continuum¶
Another useful way to think about metabolic health is as a continuum:
Optimal metabolic health → Suboptimal → Metabolic syndrome → Prediabetes → Type 2 Diabetes
This isn't a sudden cliff so much as a gradual slope. People don't wake up one day with Type 2 Diabetes; they usually slide there over years, often decades, which means there are lots of opportunities to intervene.
Research from the Whitehall II study showed that glycemia (blood sugar levels) rise slowly for about 10 years before diabetes diagnosis, then accelerate rapidly in the final two to five years before diagnosis.47
The upside is that this long lead-in creates many chances to help clients change course.
In other words, there's often a long window for intervention where lifestyle changes can slow or stop the slide, and sometimes even reverse it.
| For DIY Learners |
|---|
| Applying this to yourself: Where are you on the metabolic continuum? If you don't know, that's worth finding out. A simple fasting blood glucose and HbA1c (which your doctor can order) tell you a lot. If you're in the "suboptimal" or "prediabetes" range, the data is clear: lifestyle changes now can often prevent progression to diabetes. And if you're already diagnosed with Type 2 Diabetes, know that remission is possible for many people through intensive lifestyle changes. This isn't a one-way street. |
Why This Matters for Longevity¶
The mortality statistics are sobering. Metabolic syndrome is associated with:
- 24 percent higher all-cause mortality
- 44 percent higher heart disease mortality
- More than five-fold higher diabetes-related mortality.28
At the same time, improving metabolic health reduces these risks. In the Look AHEAD trial, participants who achieved even temporary diabetes remission had 40 percent fewer cardiovascular events and 33 percent fewer cases of chronic kidney disease compared to those who never achieved remission.19
That's why metabolic health sits at the center of longevity coaching: It's modifiable and high-impact, and coaches can make a real difference by supporting behavior change over time.
[CHONK: Insulin Resistance: The Slow Slide]
Insulin Resistance: The Slow Slide¶
Insulin resistance is often the first step on the path to Type 2 Diabetes. Understanding how it develops helps you appreciate why the lifestyle interventions you'll support actually work.
How Insulin Normally Works¶
We'll start with normal function, because it's actually pretty elegant when it works. When you eat carbohydrates:
- Your digestive system breaks carbohydrates down into glucose during digestion, so your body can use them.
- That glucose enters your bloodstream, where it raises your blood sugar for a while.
- Your pancreas senses the rise in blood sugar and releases insulin in response.
- Insulin travels through the blood and "knocks on the doors" of cells to deliver the message.
- Cells "open the door" and let glucose in, where it's used for energy.
- As glucose moves into cells, blood sugar returns to normal levels soon after.
Think of insulin as a key that opens your cells so glucose can enter. In a healthy system, the key works smoothly: glucose flows efficiently from bloodstream into cells, and everything hums along.
When this system works well, you don't even notice it; problems usually show up only when that signal starts to break down.
What Happens When Cells Become Resistant¶
Insulin resistance is when cells stop responding well to insulin's signal, so the key is in the lock but the door doesn't open as easily.
Here's what happens at the cellular level:
When cells are constantly exposed to high insulin levels (often due to frequent eating, high-sugar diets, or excess body fat), they start "turning down the volume" on their insulin receptors. It's like living next to a loud highway. Eventually, you stop hearing it.9
Several factors contribute to this resistance:
Excess fat, especially visceral fat. Fat cells aren't just storage containers; they're metabolically active, releasing hormones and inflammatory signals. Excess fat, particularly the fat stored around organs (visceral fat), releases inflammatory molecules like TNF-α and interleukins that interfere with insulin signaling.27
Ectopic fat accumulation. "Ectopic" means "in the wrong place." When fat accumulates in the liver and muscles, places it shouldn't be stored, it disrupts how these tissues respond to insulin. The liver becomes less able to suppress glucose production; muscles become less able to absorb glucose.54
Chronic inflammation. Inflammatory molecules directly interfere with the insulin signaling pathway. We'll explore this more in the inflammaging section, but the key point is: inflammation and insulin resistance fuel each other.2
Mitochondrial dysfunction. Mitochondria are tiny structures inside cells that produce energy (think of them as cellular power plants). When they don't work well, often due to inactivity, excess nutrients, or aging, cells become less efficient at processing glucose.56
The Compensation Phase¶
Here's where the body tries to fight back: when cells become resistant to insulin, the pancreas responds by producing more insulin. In other words, if the key doesn't work as well, the body tries to compensate by making more keys, a response called compensatory hyperinsulinemia.
For a while, that works, and blood sugar stays normal because there's enough extra insulin to overcome the resistance. This is why insulin resistance often exists for years before blood sugar rises enough to be detected on standard tests.
But this compensation comes at a cost: chronically high insulin levels promote fat storage and inflammation, and they may even worsen insulin resistance over time (Lewis et al., 2023).
The Progression to Type 2 Diabetes¶
Eventually, the pancreas can't keep up, and the beta cells in the pancreas, the cells that produce insulin, become exhausted. By the time someone develops impaired glucose tolerance (a stage between normal and diabetes), they've already lost 60 to 85 percent of their insulin-secreting capacity.15
The timeline varies, but research suggests a slow glycemic rise for roughly 10 years, followed by rapid deterioration in the final two to five years before diagnosis, with beta cell function declining steeply in the final five years.47
If that timeline feels intimidating, keep in mind that it also means there is usually plenty of time for clients and their medical teams to intervene. You don't need to diagnose where someone is on this curve to help them start shifting their habits.
Once both insulin resistance AND inadequate insulin production are present, Type 2 Diabetes develops.37
Early Warning Signs¶
Insulin resistance doesn't announce itself with obvious symptoms. But there are patterns clients (and their doctors) might notice:
- Feeling hungrier than usual, especially soon after meals, even if you ate “enough”
- Feeling more fatigued than usual, particularly after high-carbohydrate meals or snacks in general
- Having difficulty losing weight, and noticing more of it around the abdomen
- Noticing skin changes like dark, velvety patches in body folds (called acanthosis nigricans)
- Being diagnosed with polycystic ovary syndrome (PCOS), which is strongly linked to insulin resistance
Scope reminder: If a client describes these patterns, you can acknowledge that these symptoms are worth discussing with their doctor. You cannot tell them they have insulin resistance. That's a medical determination.
The Reversibility Window¶
The hopeful part is that insulin resistance is not a one-way street.
The same lifestyle factors that cause insulin resistance can reverse it, at least in the early stages. Weight loss, exercise, and dietary changes can restore insulin sensitivity. The earlier someone intervenes, the better their chances of preventing progression to diabetes.
Research shows that combined aerobic and resistance training reduced fasting insulin and HOMA-IR (a measure of insulin resistance) substantially in sedentary adults.44 Low-glycemic diets (those that don't spike blood sugar rapidly) also improve insulin sensitivity.55
The key message for clients: metabolic health problems develop gradually, which means there's usually time to make changes. And those changes work, which is exactly where your coaching skills can make a difference.
But here's what makes this hard¶
Knowing that metabolic health is reversible is one thing, but actually making the changes is another.
For many clients, the very metabolic dysfunction they're trying to reverse makes change harder. Insulin resistance often comes with fatigue, brain fog, and intense carbohydrate cravings, the exact symptoms that make it hard to exercise and eat differently. Their body is literally working against them.
When a client with metabolic issues "fails" to stick to a plan, this isn't weakness. It's biology. They may need smaller steps, more support, and more compassion than someone without these challenges. Your job isn't to push harder. It's to help them find a path that works despite what their body is doing.
Coaching in practice: Explaining insulin resistance to clients¶
The scenario: A client tells you their doctor mentioned "insulin resistance," and they look worried. They say, "I have no idea what that actually means, but it sounds bad."
What NOT to do:
- Launch into a long, technical lecture about receptors, mitochondria, and inflammatory molecules.
Why it doesn't work: Clients usually don't need the molecular details, and too much jargon can make them feel overwhelmed or ashamed.
What TO do:
Offer a simple, visual explanation and connect it directly to what they can do.
Sample dialogue:
Client: "My doctor said I'm insulin resistant. I don't really get what that means."
Coach: "It can definitely sound scary. Want a simple way to picture it?"
Client: "Yes, please."
Coach: "Think of insulin as a delivery person bringing packages (glucose) to your cells. When you're metabolically healthy, cells open the door right away, so delivery is smooth. With insulin resistance, cells stop opening the door as quickly, and the body responds by sending more delivery people. For a while, packages still get delivered, but eventually they start piling up in the bloodstream, which is high blood sugar. The good news is that regular movement and dietary changes are like training your cells to open the door again. They become more responsive, and the system works better."
Client: "So exercise and changing how I eat actually help my cells listen better?"
Coach: "Exactly. Exercise helps your cells become more sensitive to insulin again, and the types of foods you eat affect how much your blood sugar spikes. Over time, those changes often help people's metabolic markers improve. Your doctor can tell you what's happening with your numbers."
Key phrases that stay in scope:
- "Exercise helps your cells become more sensitive to insulin again."
- "The types of foods you eat affect how much your blood sugar spikes."
- "These changes often help people's metabolic markers improve. Your doctor can tell you what's happening with your numbers."
Phrases to avoid (out of scope):
- "Your insulin resistance is mild/moderate/severe."
- "Based on what you've told me, you probably have prediabetes."
- "You should take metformin."
[CHONK: Inflammaging: The Fire Within]
Inflammaging: The Fire Within¶
Inflammation is part of being human. But there’s a particular kind that tends to creep up with age: chronic, low-grade inflammation that can speed up aging-related processes.
Acute vs. Chronic Inflammation¶
A little context helps here, because inflammation isn’t inherently bad. It’s one of the ways your body protects you, and acute inflammation is your body’s normal response to injury or infection.
Cut your finger and the area becomes red, warm, and swollen. That’s inflammation doing its job by bringing immune cells to fight infection and repair tissue. It’s temporary, targeted, and essential for survival.
Chronic inflammation, on the other hand, is a persistent, low-level inflammatory state that doesn’t fully resolve. Instead of a fire that burns hot and then goes out, think of smoldering embers that never quite extinguish. Over time, that ongoing “heat” can damage tissues and contribute to virtually every age-related disease.40
What Is Inflammaging?¶
The term "inflammaging" combines "inflammation" and "aging." It describes the chronic, progressive, low-grade systemic inflammatory state that develops as people get older.3 In plain language, it’s background inflammation that quietly builds over time. If that sounds a bit abstract, that’s normal.
Key features of inflammaging:
- It’s chronic, meaning it tends to be “on” in the background rather than triggered by an acute infection or injury
- It’s low-grade, so you might not feel obvious symptoms, but it can still cause damage over time
- It’s systemic, affecting the whole body, not just one location
- It’s progressive, and it tends to worsen with age unless actively addressed
Inflammaging has been linked to frailty, disability, cognitive decline, cardiovascular disease, Type 2 Diabetes, neurodegeneration, and mortality.50
The Mechanisms Behind Inflammaging¶
So where does this “slow burn” come from? Inflammaging is driven by several interconnected processes that stack on top of each other over time:
Cellular senescence and SASP. As cells age, some enter a state called senescence, where they stop dividing but don’t die. These “zombie cells” release inflammatory molecules (collectively called the Senescence-Associated Secretory Phenotype, or SASP). The more senescent cells accumulate, the more inflammation they produce.4 “Zombie cells” is a common nickname in the research.
Mitochondrial dysfunction. Remember those cellular power plants? When mitochondria malfunction, they produce reactive oxygen species (ROS), unstable molecules that damage cells and trigger inflammatory pathways.56
Gut microbiome changes. As people age, their gut bacteria change, with less diversity and more pro-inflammatory species. The gut barrier can also become more permeable (sometimes called "leaky gut"), which allows bacterial products to enter the bloodstream and trigger inflammation.7
Immune system changes (immunosenescence). The immune system becomes less efficient with age, but paradoxically more prone to producing inflammatory signals. It’s like a security system that keeps setting off false alarms while also missing actual threats.50
NF-κB and inflammasome activation. These are molecular pathways that, when chronically activated, drive sustained inflammation. Various age-related stressors (damaged DNA, misfolded proteins, mitochondrial dysfunction) can trigger these pathways.29
| For DIY Learners |
|---|
| Applying this to yourself: Inflammaging isn’t just academic. It’s happening to all of us to some degree as we age. The real question is whether your day-to-day habits are adding fuel or helping to cool things down. Sleep deprivation, chronic stress, poor diet, sedentary behavior, and excess body fat all fan the flames. On the flip side, exercise, adequate sleep, stress management, and anti-inflammatory nutrition (think Mediterranean diet patterns) help damp them down. If you're wondering whether you have chronic inflammation, a simple hsCRP test (which your doctor can order) can give you a general sense. But regardless of your numbers, those lifestyle interventions still help. |
If all these pathways and acronyms feel like alphabet soup, that’s OK. You don’t need to memorize each mechanism. What matters is the big idea: many age-related processes nudge the body toward a chronic, simmering inflammatory state, and your habits can shift that trend over time.
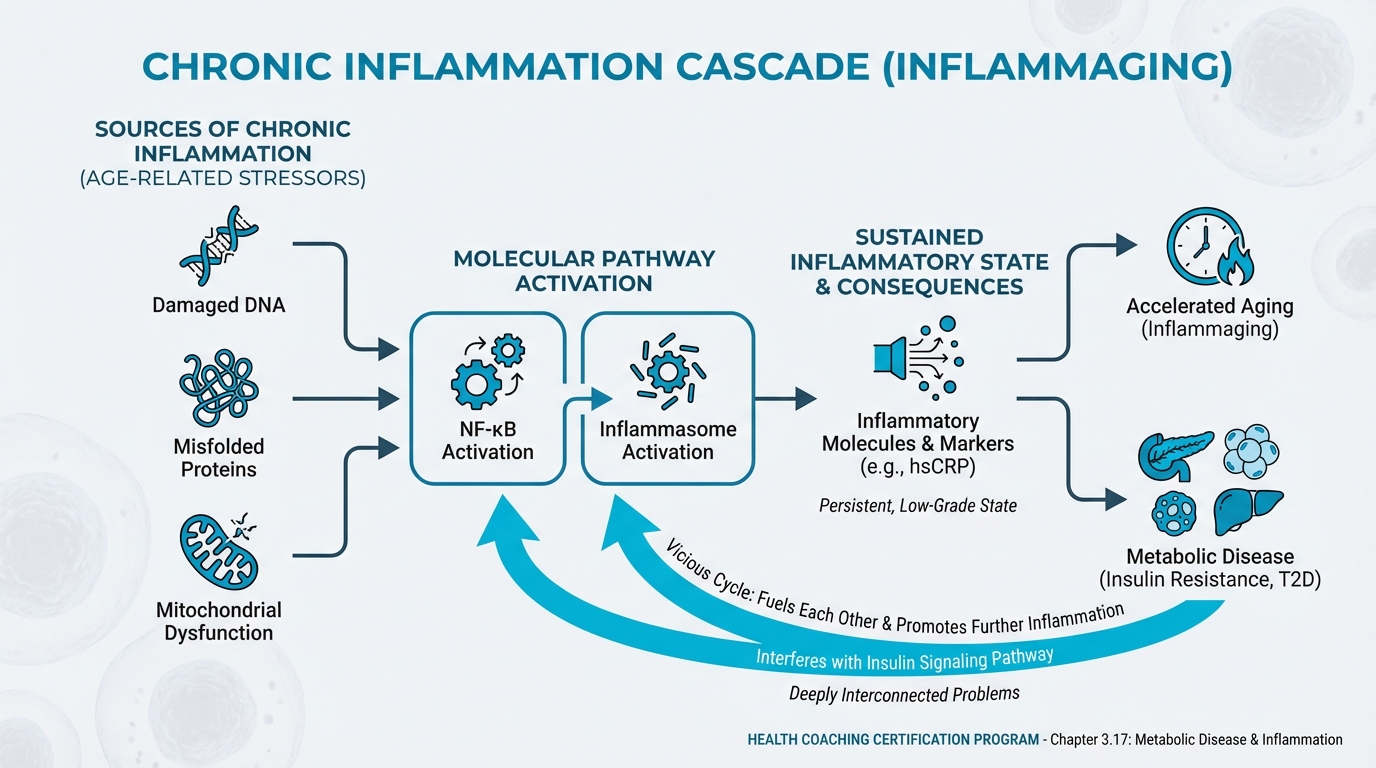
Figure: Chronic inflammation pathways
Inflammation Biomarkers¶
Inflammation can be measured with blood tests. The most common is hsCRP (high-sensitivity C-reactive protein), a protein the liver produces in response to inflammation, measured in milligrams per liter (mg/L).
General hsCRP ranges (for educational purposes only):
- Less than 1.0 mg/L: lower cardiovascular risk
- 1.0-3.0 mg/L: moderate risk
- Greater than 3.0 mg/L: higher risk.39
Critical scope reminder: You cannot interpret a client's hsCRP results or tell them their inflammation is "high" or "low." If a client shows you their test results, you can explain what hsCRP measures in general terms, but interpretation belongs to their physician. This boundary can feel a little awkward at first, and it gets easier with practice.
Other inflammation-related markers doctors may assess include ESR (erythrocyte sedimentation rate), IL-6 (interleukin-6), and TNF-α (tumor necrosis factor alpha). Again, interpretation is medical scope.
What the Research Shows About hsCRP and Mortality¶
The research connecting inflammation to mortality is sobering:
- In the UK Biobank study (more than 400,000 people), those in the highest CRP quartile had 68 percent higher risk of premature death compared to the lowest quartile.31
- In a Shanghai cohort, CRP above 3 mg/L was associated with 53 percent higher all-cause mortality and 71 percent higher cardiovascular mortality compared to CRP under 1 mg/L.23
- A composite inflammaging score predicted mortality (41 percent higher risk per standard deviation increase) independent of epigenetic aging measures.12
- ESR between 20-50 mm/hr predicted 23 percent higher mortality compared to ESR under 20; ESR above 50 predicted 89 percent higher mortality.16
Taken together, these statistics show why reducing chronic inflammation matters for longevity.
If all of those risk percentages are starting to blur together, you’re not alone. The takeaway is simple: higher levels of chronic inflammation consistently track with higher risk of disease and early death.
Sources of Chronic Inflammation¶
Inflammaging isn’t just about aging itself. Lifestyle factors can play a big role too, and this is where clients often have real room to make progress.
Diet. Western dietary patterns (high in processed foods, refined sugars, and saturated fats) activate inflammatory pathways. These foods increase gut permeability, alter the microbiome, and directly trigger inflammatory signaling.33
Obesity, especially visceral fat. Fat tissue actively produces inflammatory molecules. Generally, the more excess fat (particularly abdominal fat), the more inflammation.41
Sedentary behavior. Physical inactivity increases inflammatory markers, while regular exercise is one of the most powerful anti-inflammatory interventions available.22
Chronic stress. Sustained psychological stress activates the HPA axis and sympathetic nervous system, shifting immune function toward pro-inflammatory states. Stress hormones activate inflammatory pathways including NF-κB.32
Poor sleep. Sleep deprivation increases inflammatory markers. This connects to your learning from the sleep chapters, because sleep isn’t just about energy. It’s also one of the ways the body keeps inflammation in check.
Smoking. Smokers show higher CRP, IL-6, and other inflammatory markers. Even after quitting, some elevation may persist.14
Gut dysbiosis. Imbalanced gut bacteria can increase intestinal permeability, allowing bacterial products (particularly lipopolysaccharides, or LPS) to enter circulation and trigger systemic inflammation.8
What Coaches Can Do¶
This is where your role becomes practical and clear. You cannot diagnose inflammation or interpret test results, but you can support clients in the parts they control.
In practice, that can look like:
- Educating clients about inflammation as a modifiable factor in aging
- Supporting behavior changes that reduce inflammation (movement, dietary quality, sleep, stress management)
- Encouraging clients to discuss inflammation concerns with their medical providers
- Helping clients implement anti-inflammatory recommendations from their healthcare team
Here’s what that sounds like in real life.
What NOT to do (out of scope)
Client: “My hsCRP is 3.4, and I’m wondering if that’s bad?”
Coach: “Yes, that’s high, and you need to get it down; start taking omega-3s and cut out gluten, dairy, and sugar.”
A better coaching approach (in scope)
Client: “My hsCRP is 3.4, and I’m wondering if that’s bad?”
Coach: “Thanks for sharing that. I can explain what hsCRP measures in general, but I can’t interpret your result, so it’s best to review it with your physician. Have you had a chance to do that yet?”
Client: “Not yet, and I’m just worried.”
Coach: “That makes sense. While you follow up with them, we can work on the lifestyle pieces that tend to support healthier inflammation levels: consistent movement, sleep, food quality, and stress management. Which of those feels most doable to start with this week?”
If you’re thinking, “Okay, but where do I start with a real human who’s busy and stressed?”, you’re asking the right question. Start with the fundamentals and build from there. Simple doesn’t always mean easy.
[CHONK: Lifestyle Reversal: It's Not Too Late]
Lifestyle Reversal: It's Not Too Late¶
If metabolic disease and inflammation sound like inevitable consequences of aging, the hopeful counter-narrative is that substantial evidence shows these conditions can be improved, and sometimes reversed, through lifestyle changes.
The DiRECT Trial: A Landmark Study¶
The Diabetes Remission Clinical Trial (DiRECT) changed how we think about Type 2 Diabetes. Researchers enrolled people with Type 2 Diabetes (diagnosed within the previous six years) and put the intervention group through an intensive diet program using total diet replacement (very low calorie).
Results:
- 46 percent achieved remission at one year (intervention) vs. 4 percent (control).24
- 36-40 percent remained in remission at two years.52,11
- 13 percent were still in remission at five years.13
The dose-response relationship with weight loss was striking. At one year:
- Less than 5 kg lost: 7 percent remission
- 5-10 kg lost: 34 percent remission
- 10-15 kg lost: 57 percent remission
- 15+ kg lost: 86 percent remission.24
If all those percentages are starting to blur together, that's completely fine. The key idea is that greater, sustained weight loss generally means a higher chance of remission, especially earlier in the disease process.
What "remission" means: HbA1c under 6.5 percent (or fasting glucose under 126 mg/dL) without diabetes medications for at least two months. Remission doesn't mean "cured." The underlying susceptibility remains, and weight regain typically brings blood sugar back up.
The Mechanisms of Reversal¶
Research has clarified why weight loss reverses Type 2 Diabetes:
Liver fat reduction. After just one week of very low calorie diet, fasting glucose normalized and hepatic (liver) insulin sensitivity improved. The liver was releasing less glucose into the bloodstream.30
Pancreatic fat reduction. Pancreatic fat dropped from about 8 percent to 6.2 percent after eight weeks, and first-phase insulin secretion more than doubled.30 The pancreas was recovering function.
Restored beta cell function. The insulin-producing cells, previously overwhelmed, began functioning better as the metabolic stress lifted.46
The key insight: Type 2 Diabetes isn't a fixed state. In many cases, it reflects overwhelmed metabolic machinery that can recover when the burden is lightened.
Beyond DiRECT: What Works for Metabolic Improvement¶
While DiRECT used intensive total diet replacement, other interventions also improve metabolic health:
Exercise, especially combined training. A meta-analysis found combined aerobic and resistance training reduced fasting insulin by about 1.0 standard deviation and HOMA-IR (insulin resistance measure) by about 0.95 standard deviations in sedentary adults.44 That's a meaningful improvement.
The ACSM consensus statement notes that moderate-intensity aerobic training lowers HbA1c by approximately 0.5-0.7 percent in people with Type 2 Diabetes.1
Diet + exercise outperforms diet alone. A randomized trial showed that adding exercise to a weight-loss diet produced about twice the improvement in whole-body insulin sensitivity compared to diet alone, at the same amount of weight loss.6 Exercise provides benefits beyond just what the scale shows.
Dietary patterns matter. Low-glycemic index diets (those that don't spike blood sugar rapidly) significantly improve insulin resistance compared to high-glycemic diets.55 Mediterranean-style diets, rich in vegetables, olive oil, and fish, improve multiple metabolic markers and reduce Type 2 Diabetes risk.38
Time-restricted eating. As you learned in Chapter 2.8, TRE can improve glucose homeostasis. Research in animals shows TRE can restore the daily oscillations in respiratory exchange ratio (a measure of fuel switching) even without weight loss.53 Fasting periods longer than 12 hours shift metabolism toward fat burning and may trigger beneficial cellular cleanup processes like autophagy.35
Gut health interventions. Meta-analyses show probiotics and prebiotics produce modest but significant improvements in glycemic markers in people with Type 2 Diabetes, including reductions in HbA1c, fasting glucose, and HOMA-IR.49
Anti-Inflammatory Lifestyle Interventions¶
For reducing chronic inflammation, the evidence points to:
Exercise, the most consistent evidence. A meta-analysis of aerobic exercise in older adults found significant reductions in CRP (about 0.85 mg/L), IL-6, and TNF-α, along with increases in anti-inflammatory IL-10.48 Lifelong exercisers have lower baseline inflammatory markers than sedentary peers.42
Mediterranean dietary patterns. A 2025 meta-analysis of randomized trials found that Mediterranean diets significantly improved hsCRP, IL-6, and IL-17.36 The pattern matters more than any single food.
Mind-body practices. Meta-analyses show yoga, meditation, and Tai Chi decrease pro-inflammatory cytokines.34,25
Weight loss. Reducing excess body fat, especially visceral fat, reduces the inflammatory signals emanating from adipose tissue.
Curcumin supplementation. Curcumin, the active compound in turmeric, has anti-inflammatory properties supported by multiple meta-analyses showing reductions in CRP and other inflammatory markers. The longevity protocol references 1g daily with black pepper (piperine) to enhance absorption. However, curcumin is a supplement, meaning it's "extra credit" after the lifestyle fundamentals above are in place. Anyone interested should discuss with their healthcare provider, especially if taking medications that affect blood clotting. (See Chapter 3.15 for more on supplements.)
Complications Reduction in Look AHEAD¶
The Look AHEAD trial followed over 5,000 people with Type 2 Diabetes through an intensive lifestyle intervention focused on weight loss. While the trial didn't show a significant reduction in cardiovascular events overall, secondary analyses revealed important findings:
- Participants who achieved any remission had 40 percent fewer cardiovascular events (HR 0.60).
- They also had 33 percent fewer cases of chronic kidney disease (HR 0.67).19
Even short-term remission conferred benefit. This underscores that metabolic improvement, even if not permanent, matters for long-term outcomes.
If those outcomes make you worry that you have to produce "trial-level" results with every client, take a breath. You're not trying to recreate a research study; you're helping real people make meaningful, sustainable changes in the context of their actual lives. (That's enough.)
Setting Realistic Expectations¶
While the evidence for lifestyle reversal is strong, it's important to be realistic with clients:
Durability requires maintenance. In DiRECT, among those in remission at two years, only about 26 percent remained in remission at five years.18 Weight regain typically leads to blood sugar returning to diabetic levels.
Not everyone responds equally. Longer diabetes duration and greater loss of beta cell function predict lower likelihood of remission.17 Earlier intervention works better.
Lifestyle changes require support. The intensive support in DiRECT and Look AHEAD contributed to outcomes. Real-world implementation without that support may show smaller effects.
If that sounds a bit discouraging, remember that even temporary improvements in blood sugar and weight can reduce complications and buy people more healthy years. Progress still counts, even if remission isn't permanent.
This is where you come in. Your role as a coach, helping clients maintain changes over time, is exactly what's needed to translate trial results into real-world impact.
Your job isn't to guarantee remission; it's to help clients make sustainable changes that move them in a better direction over time.
Coaching in practice: The hierarchy of metabolic interventions¶
The scenario: A client with newly diagnosed prediabetes says, "Just tell me which supplements and gadgets I need to fix this," but they're sleeping five hours a night, barely moving, and eating most meals from a drive-thru.
What NOT to do:
- Start with third-tier "biohacks" like supplements while ignoring foundations.
- Overwhelm them with a dozen simultaneous changes.
Why it doesn't work: This majors in the minors and often leaves clients frustrated when the basics would have had the biggest impact.
What TO do:
Lay out a clear hierarchy so you focus first on what moves the needle most.
First tier, strongest evidence:
- Weight management (if excess weight is present): remission rates directly correlate with weight loss.
- Regular movement. Both aerobic and resistance training improve insulin sensitivity.
- Dietary pattern quality: less processed food, more vegetables, appropriate portions.
Second tier. Supportive evidence:
- Meal timing and composition (post-meal walks, protein/fiber first, time-restricted eating).
- Sleep optimization. Poor sleep worsens insulin resistance.
- Stress management. Chronic stress elevates blood sugar and inflammation.
Third tier. Emerging/modest evidence:
- Specific gut health interventions (fermented foods, fiber diversity).
- Anti-inflammatory foods (beyond general dietary quality).
Sample dialogue:
Client: "Just tell me which supplements and gadgets I need to fix this. I don't have time to overhaul my whole life."
Coach: "I get wanting a clear, simple answer. Before we talk about extras like supplements, would it be OK if I showed you what tends to make the biggest difference for blood sugar in real people?"
Client: "Sure, I guess."
Coach: "Think of this like a pyramid. The base is things like sleep, movement, and what you're eating most days. Right now you're sleeping about five hours, barely moving, and grabbing most meals from the drive-thru. If we put your energy into supplements before we touch those foundations, it's kind of like putting fancy rims on a car without fixing the engine."
Client: "So you're saying the basics will move the needle more than the gadgets?"
Coach: "Exactly. Once we get your sleep, movement, and meals working better for you, then if you still want to explore add-ons, we can do that alongside your doctor. Starting with the foundations gives you the best return on your effort."
Critical reminder: You support these interventions through behavior change coaching. The medical team monitors results, adjusts medications, and determines whether metabolic goals are being met.
[CHONK: Coaching Metabolic Health (Within Scope)]
Coaching Metabolic Health Within Scope¶
Metabolic health is one of those areas where coaching can make a real difference, and scope boundaries matter a lot at the same time. So how do you support clients with metabolic concerns while staying firmly within your scope of practice?
If you ever feel a bit anxious about overstepping, that's actually a good sign because it usually means you're paying attention to your professional boundaries. (That kind of care is part of being a pro.)
What Coaches CAN Do¶
Educate about metabolic health. You can explain what insulin resistance is, how blood sugar works, and what inflammation means, using clear, everyday language. The educational content in this chapter helps clients understand why lifestyle changes matter in the first place.
Support lifestyle change implementation. This is your core function, and it’s often where coaches have the biggest impact. When a client's doctor says, "you need to lose weight" or "increase your activity," you help make that happen through goal-setting, habit formation, barrier troubleshooting, and accountability. These are coaching skills that translate directly to metabolic health improvement. (This is where coaches really shine.)
Encourage and support medical recommendations. If a physician prescribes metformin, you can help the client build reminders and routines, and then bring side effects back to their medical team. And if a dietitian creates a meal plan, you can help the client follow it consistently in real life.
Facilitate behavior change conversations. Motivational interviewing helps clients explore their own reasons for change, which tends to work better than you trying to “convince” them. For example: "What matters most to you about improving your metabolic health?" and "What would be different in your life if your blood sugar were better controlled?"
Help clients prepare for medical appointments. You can help clients write down questions, track their habits (so they can report accurately to their doctor), and then process what they heard after the appointment. (This is especially helpful when clients leave visits feeling rushed or overwhelmed.)
Coordinate with the medical team (with consent). With client permission, you can communicate with physicians, share observations about client progress, and help ensure everyone is on the same page.
What Coaches CANNOT Do¶
Diagnose metabolic conditions. If a client says, "I think I have insulin resistance," you cannot confirm or deny. A scope-safe response is: "That's worth discussing with your doctor. They can run the appropriate tests."
Interpret lab results. If a client shows you their glucose, HbA1c, or triglyceride results, you cannot tell them if their numbers are "good" or "bad." You can explain, in general terms, what these tests measure, but interpretation is medical scope. "Your doctor is the best person to tell you what these results mean for you specifically."
Recommend supplements for metabolic conditions. You cannot tell a client to take berberine, chromium, cinnamon, or any other supplement for blood sugar management. Even natural supplements can interact with medications and affect metabolic function. (This is one of those “sounds harmless, can be complicated” areas.)
A special note on berberine: This supplement has significant research showing glucose-lowering effects similar to diabetes medications. Fasting glucose reductions of about 0.5-0.8 mmol/L and HbA1c reductions of about 0.4-0.7 percent across meta-analyses.51,10 Because of this medication-like effect, berberine is firmly in medical scope. If clients ask about it, you can say: "Berberine has research behind it, but because it affects blood sugar similarly to some medications, it's something to discuss with your doctor, especially if you're on any medications."
Recommend medication changes. You cannot suggest clients start, stop, or change diabetes medications. Even "you should talk to your doctor about reducing your medication," while well-intentioned, crosses into medical decision-making.
Provide medical nutrition therapy. Individualized meal planning for metabolic disease management requires a registered dietitian. You can support general healthy eating patterns and help clients follow dietitian-created plans, but creating therapeutic diets is outside coaching scope.
If this line between “coach” and “clinician” feels a little strict, you’re not alone, and it’s normal. It also gets easier with practice. (If you’re ever unsure, looping in the client’s medical team is a safe move.)
Supporting Clients WITH Type 2 Diabetes¶
Many of your clients will already have a Type 2 Diabetes diagnosis, and to be clear, you're not treating their diabetes; their medical team does that.
What you can provide (and what medical appointments often can't) is steady, consistent support between visits. Here’s what that can look like:
Help them implement lifestyle changes their medical team recommends. Most diabetes treatment plans include lifestyle components, and you're the person who helps make those happen, not by prescribing, but by supporting the doing.
Support medication adherence. If remembering medications is challenging, you can help with systems and accountability, always in support of, not instead of, their medical plan.
Address the emotional component. A diabetes diagnosis can bring shame, fear, and denial. (These reactions are more common than most people realize.) You can offer a supportive space to talk it through, while referring to mental health professionals if distress is significant.
Celebrate progress. When their doctor reports improved HbA1c, acknowledge the behavior changes that likely contributed. "Your consistency with those post-dinner walks is really showing up," and that matters more than you might think.
Navigate setbacks without judgment. Blood sugar management has ups and downs. That's reality, not failure, so help clients learn from setbacks rather than spiraling into self-criticism. (This is a skill, and it takes practice.)
When to Refer¶
Some situations require immediate medical referral:
Red flags that require urgent physician contact:
- Symptoms of very high blood sugar (extreme thirst, frequent urination, blurred vision, unexplained weight loss)
- Symptoms of very low blood sugar (shakiness, confusion, sweating, rapid heartbeat), especially if client is on glucose-lowering medication
- Signs of diabetic ketoacidosis (fruity breath, nausea/vomiting, confusion, abdominal pain)
- Non-healing wounds or sores, especially on feet
- Sudden vision changes
- Chest pain, shortness of breath, or other cardiovascular symptoms
Situations requiring physician follow-up:
- Client hasn't seen their doctor about metabolic concerns in the past year
- Client reports significant changes in their condition
- Client wants to change their medication or supplement regimen
- Client's lifestyle changes are producing rapid improvements (medication may need adjustment to prevent low blood sugar)
- Client expresses interest in pursuing diabetes remission
CGM in Coaching: A Special Consideration¶
Continuous glucose monitors (CGMs) are increasingly available over-the-counter, and some non-diabetic clients use them for optimization purposes. If a client uses a CGM, scope considerations still apply.
What you can do:
- Help them notice patterns (e.g., "what do you observe about your glucose after different types of meals?")
- Support behavior experiments they design (e.g., "let's see what happens when you take a walk after dinner")
- Provide education about normal glucose variation in healthy people
What you cannot do:
- Interpret whether their glucose patterns indicate pathology
- Diagnose insulin resistance or prediabetes based on CGM data
- Make supplement or medication recommendations based on glucose data
Important context: Healthy adults on CGM typically spend about 96 percent of time in the 70-140 mg/dL range, with about 1 percent of time briefly below 70 mg/dL. These brief dips are often clinically insignificant.43,45 Overmonitoring can cause unnecessary anxiety. Some research on wearable health devices shows a subset of users develop monitoring-related anxiety, a phenomenon called "orthosomnia" for sleep trackers.5,21
If a client seems anxious about their CGM data, that's worth addressing. (And if you've ever felt this way looking at your own wearable data, you're in good company.) Data should empower, not stress.
Professional Language¶
The words you choose matter. Here are scope-safe ways to talk about metabolic topics without diagnosing, interpreting, or prescribing:
-
Instead of: "Your blood sugar is too high."
Try: "How did your doctor explain your blood sugar results?" -
Instead of: "You have insulin resistance."
Try: "It sounds like your doctor mentioned some metabolic concerns. What did they recommend?" -
Instead of: "You should take chromium for blood sugar."
Try: "Any supplements that affect blood sugar are worth discussing with your doctor first." -
Instead of: "Based on what you've told me, I think you're prediabetic."
Try: "Those symptoms are worth mentioning to your doctor. They can run tests to see what's going on." -
Instead of: "You're doing great. Your inflammation is probably down."
Try: "You've been really consistent with these changes. Your doctor can check how your markers are responding at your next visit."
Coaching in practice: 'I think I have diabetes'¶
The scenario: A client tells you, "I think I have diabetes. I'm always tired after meals."
What NOT to do:
- "Yes, that sounds like diabetes. You probably have blood sugar issues." (This is diagnosing.)
- "You should cut all carbs." (This is prescriptive nutrition.)
- "Take some berberine. It helps with blood sugar." (This is supplement recommendation for a medical condition.)
What TO do:
Validate their concern, encourage medical evaluation, and shift into pattern exploration, without giving a diagnosis.
Sample dialogue:
Client: "I think I have diabetes. I'm always tired after meals."
Coach: "Feeling wiped out after you eat can definitely be frustrating. It's also something your doctor will want to know about, because they can run tests to see what's going on."
Client: "So you think I have diabetes?"
Coach: "I can't say what is or isn't going on. That's your doctor's role. What I can do is help you notice patterns so you have good information to share. For example, have you noticed whether certain meals make you more tired than others?"
Client: "Yeah, big pasta lunches seem to knock me out."
Coach: "That's really useful to know. Let's track that for a bit so you and your doctor have clearer data to work with, and we can experiment with meals that leave you feeling more steady."
Why this stays in scope:
- Doesn't diagnose
- Encourages medical evaluation
- Offers coaching support (pattern exploration) that stays in scope
[CHONK: Deep Health Integration]
Deep Health Integration¶
Metabolic health and inflammation touch all six dimensions of Deep Health. Here’s how the connections tend to show up:
Physical¶
This is the primary dimension because metabolic function is a physical process, and insulin sensitivity, glucose regulation, and inflammation all show up in the body. The physical dimension includes:
- Body composition, including muscle mass and where you tend to store body fat
- Cardiovascular function, since metabolic disease increases CVD risk over time
- Day-to-day energy levels, because metabolic dysfunction often shows up as fatigue
- Sleep quality (poor sleep worsens insulin resistance; poor metabolic health worsens sleep)
Mental¶
Blood sugar fluctuations affect cognitive function, and research shows that:
- High glucose variability is associated with worse cognitive performance
- Both hypoglycemia (low blood sugar) and hyperglycemia (high blood sugar) can cause mental fog
- Chronic inflammation is linked to cognitive decline and neurodegeneration
For your clients, this might manifest as difficulty concentrating, brain fog after meals, or mental fatigue. These are worth noting and worth sharing with their medical team. You don't need to have all the answers about why a client feels foggy; noticing patterns and encouraging follow-up is enough.
Emotional¶
Metabolic disease brings emotional complexity:
- Shame: Many people feel embarrassed about metabolic diagnoses, especially given societal stigma around weight
- Fear: Worries about disease progression, potential complications, or what “diabetes” could mean for them
- Denial: Minimizing concerns, especially when symptoms don’t feel urgent yet
- Frustration: Feeling stuck when lifestyle changes don’t produce immediate, visible results
- Food anxiety: Getting so focused on monitoring that eating starts to feel stressful or rigid
Your role includes holding space for these emotions, normalizing them, and helping clients separate their identity from their metabolic status. If you're not always sure exactly what to say, that's OK; simply listening and validating can be extremely powerful.
Social¶
Social factors profoundly influence metabolic health, often in ways clients don’t see at first:
- Food environment: Family meals, workplace snacks, and the social norms around eating
- Support systems: Supportive friends and family can make lifestyle changes easier to stick with
- Social determinants: Access to healthy food, safe places to exercise, and consistent healthcare
- Social comparison: Watching others “eat whatever they want” while they’re working on blood sugar
Social eating is particularly relevant. Help clients develop strategies for navigating social situations without feeling isolated or deprived.
What not to do
Client: "I’m trying to get my blood sugar under control, but every weekend is dinners and drinks with friends."
Coach: "Then you’ll need to stop going out or you’ll never make progress."
A better approach
Client: "I’m trying to get my blood sugar under control, but every weekend is dinners and drinks with friends."
Coach: "That makes sense. Social plans are a big part of life. Want to walk through what usually happens on those nights and find one or two small changes that still let you enjoy the time with friends?"
Environmental¶
This often gets overlooked: the built environment shapes metabolic health in powerful ways.
- Food environment: Proximity to grocery stores vs. fast food, food deserts
- Physical activity infrastructure: Walkability, parks, gym access
- Work environment: Desk jobs, shift work (which disrupts circadian rhythms and worsens metabolic health)
- Toxin exposure: Some environmental chemicals (endocrine disruptors) may contribute to metabolic dysfunction
You can't change a client's environment single-handedly, but you can help them see it clearly. Often, just naming environmental barriers takes away some of their power. And together, you can brainstorm workarounds.
Existential¶
Metabolic health connects to bigger-picture concerns:
- Longevity and mortality: Clients may confront their own mortality when diagnosed with metabolic disease
- Quality of life: Fear of complications (blindness, amputation, kidney failure) looms large
- Purpose and identity: "Am I going to be 'a diabetic' forever?"
- Future planning: Concerns about being healthy for children, grandchildren, retirement
These existential dimensions can be powerful motivators for change, or sources of overwhelming despair. Help clients connect their daily choices to their larger values and purposes.
You're not acting as a therapist here, but you can listen, reflect what you hear, and, when appropriate, suggest mental health support. (You don't have to carry this alone.)
[CHONK: Case Study]
Case Study: Marcus¶
Client Profile:
Marcus, 54, was recently told by his doctor that he has "prediabetes" with an HbA1c of 6.1 percent. His doctor also mentioned his hsCRP was "a little elevated" at 2.8 mg/L. Marcus was given a pamphlet about diet and exercise and told to come back in six months. He found a longevity coach (you) because he doesn't want to "become diabetic like my father." (Understandably.)
What Marcus shares:
- Works long hours at a desk job and feels "constantly stressed" about work
- Eats most meals on the go or at restaurants, so he has limited meal control
- Hasn't exercised regularly in years, so he gets winded climbing stairs, and he typically sleeps about 5-6 hours per night
- Drinks alcohol socially, 2-3 nights per week, and his waist circumference is 42 inches
Initial Coach Response:
You recognize several factors that contribute to metabolic dysfunction and inflammation: sedentary work, poor sleep, stress, possible excess visceral fat, and limited meal control, which are all coachable areas.
You also recognize your boundaries: you won't tell Marcus his numbers are "bad," diagnose insulin resistance, or prescribe a treatment plan; you'll support behavior change.
First Session Approach:
You start with values exploration by asking: "What matters most to you about your health right now?"
Marcus talks about his father's diabetes complications (foot amputation) and wanting to be healthy for his kids. That’s powerful motivation material, and it gives you a clear place to start.
You ask: "What did your doctor recommend, and what do you think might be most helpful right now?"
Marcus admits the pamphlet felt generic. (We hear that a lot.) He knows he "should eat better and exercise more" but doesn't know where to start.
Collaborative Planning:
Rather than prescribing, you explore: "If you were going to make one change this week, what feels most doable?"
Marcus decides that eating breakfast at home instead of grabbing a muffin is something he could try.
You help make this specific by asking: What breakfast will it be, when will he eat it, what needs to be in the house, and what might get in the way?
Progress Over Time:
Over several months, Marcus:
- Starts with a 15-minute post-dinner walk and builds it to 30 minutes
- Shifts breakfast and lunch toward higher protein and more vegetables
- Starts strength training twice weekly with a trainer
- Prioritizes seven hours of sleep on weekdays and reduces alcohol to weekends only
Six-Month Follow-Up:
Marcus returns to his doctor. His HbA1c has dropped to 5.8 percent (no longer in prediabetes range), and his hsCRP is now 1.4 mg/L. He's lost 12 pounds, mostly from the midsection.
If these changes sound simple but powerful, that's the point: small, consistent shifts can add up.
What the Coach Did Well:
- Supported medical recommendations while staying in scope, and let the doctor interpret lab results
- Used client values as a motivation anchor, then started with small, achievable changes and built gradually from there
- Celebrated the process (behavior changes), not just outcomes (lab results), and connected Marcus with a trainer for the exercise component
What the Coach Didn't Do:
- Didn't diagnose or confirm prediabetes, interpret lab values, or tell Marcus to stop his doctor-prescribed plan
- Didn't recommend supplements or create a meal plan (helped with behavioral strategies instead)
[CHONK: Study guide questions]
Study Guide Questions¶
Here are some questions to help you think through the material and prepare for the chapter exam. They're optional, but we recommend answering at least a few as part of your active learning process.
-
What is insulin resistance, and what are the key factors that contribute to its development?
-
What does "inflammaging" mean, and why is it relevant to longevity coaching?
-
What were the key findings of the DiRECT trial regarding Type 2 Diabetes remission?
-
A client shows you their blood work and asks "Is my A1C good?" How do you respond while staying in scope?
-
What are three lifestyle interventions with strong evidence for improving metabolic health?
-
Why might a supplement like berberine be outside coaching scope to recommend?
-
How does chronic inflammation connect to metabolic dysfunction?
-
What red flags in a client with metabolic concerns should prompt immediate medical referral?
Self-reflection questions:
-
Pay attention to your energy after meals this week: do you crash 2-3 hours after eating certain foods, and if so, what patterns do you notice?
-
What's your waist circumference, and what might it tell you about your metabolic health compared to scale weight alone?
Works cited¶
References¶
-
ACSM. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement. Med Sci Sports Exerc; 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC8802999/
-
Ahn B. Advances in Insulin Resistance—Molecular Mechanisms, Therapeutic Targets, and Future Directions. International Journal of Molecular Sciences. 2025;26(6):2574. doi:10.3390/ijms26062574
-
Andonian BJ, Hippensteel JA, Abuabara K, Boyle EM, Colbert JF, Devinney MJ, et al. Inflammation and aging-related disease: A transdisciplinary inflammaging framework. GeroScience. 2024;47(1):515-542. doi:10.1007/s11357-024-01364-0
-
Baechle JJ, Chen N, Makhijani P, Winer S, Furman D, Winer DA. Chronic inflammation and the hallmarks of aging. Molecular Metabolism. 2023;74:101755. doi:10.1016/j.molmet.2023.101755
-
Baron KG, Abbott S, Jao N, Manalo N, Mullen R. Orthosomnia: Are Some Patients Taking the Quantified Self Too Far?. Journal of Clinical Sleep Medicine. 2017;13(02):351-354. doi:10.5664/jcsm.6472
-
Beals JW, Kayser BD, Smith GI, Schweitzer GG, Kirbach K, Kearney ML, et al. Dietary weight loss-induced improvements in metabolic function are enhanced by exercise in people with obesity and prediabetes. Nature Metabolism. 2023;5(7):1221-1235. doi:10.1038/s42255-023-00829-4
-
Caldarelli M, Rio P, Marrone A, Giambra V, Gasbarrini A, Gambassi G, et al. Inflammaging: The Next Challenge—Exploring the Role of Gut Microbiota, Environmental Factors, and Sex Differences. Biomedicines. 2024;12(8):1716. doi:10.3390/biomedicines12081716
-
Cani PD, Amar J, Iglesias MA, Poggi M, Knauf C, Bastelica D, et al. Metabolic Endotoxemia Initiates Obesity and Insulin Resistance. Diabetes. 2007;56(7):1761-1772. doi:10.2337/db06-1491
-
Chandrasekaran P, Weiskirchen R. Cellular and Molecular Mechanisms of Insulin Resistance. Current Tissue Microenvironment Reports. 2024;5(3):79-90. doi:10.1007/s43152-024-00056-3
-
Cheung AWL, et al. Overall and Sex-Specific Effect of Berberine on Glycemic and Insulin-Related Traits: A Systematic Review and Meta-Analysis. J Nutr; 2023. https://pubmed.ncbi.nlm.nih.gov/37598753/
-
Corrao S, Falcone F, Mirarchi L, Amodeo S, Calvo L. Type 2 Diabetes Mellitus Remission, Dream or Reality? A Narrative Review of Current Evidence and Integrated Care Strategies. Diabetes Therapy. 2025;16(8):1557-1579. doi:10.1007/s13300-025-01761-4
-
Cribb L, Hodge AM, Yu C, Li SX, English DR, Makalic E, et al. Inflammation and Epigenetic Aging Are Largely Independent Markers of Biological Aging and Mortality. The Journals of Gerontology: Series A. 2022;77(12):2378-2386. doi:10.1093/gerona/glac147
-
Diabetes UK. Weight loss can put type 2 diabetes into remission for at least five years, DiRECT study reveals. Press release; 2024. https://www.diabetes.org.uk/about-us/news-and-views/weight-loss-can-put-type-2-diabetes-remission-least-five-years-reveal-latest-findings
-
Elisia I, Lam V, Cho B, Hay M, Li MY, Yeung M, et al. The effect of smoking on chronic inflammation, immune function and blood cell composition. Scientific Reports. 2020;10(1). doi:10.1038/s41598-020-76556-7
-
Feingold KR, et al. Pathogenesis of Type 2 Diabetes Mellitus. Endotext; 2024. https://www.ncbi.nlm.nih.gov/books/NBK279115/
-
Fest J, Ruiter R, Mooijaart S, Ikram MA, van Eijck CHJ, Stricker BH. Erythrocyte sedimentation rate as an independent prognostic marker for mortality: a prospective population‐based cohort study. Journal of Internal Medicine. 2018;285(3):341-348. doi:10.1111/joim.12853
-
Ghusn W, Hurtado MD, Acosta A. Weight-centric treatment of type 2 diabetes mellitus. Obesity Pillars. 2022;4:100045. doi:10.1016/j.obpill.2022.100045
-
Glasgow University. Diet intervention links longer remissions of type 2 diabetes and improved health over 5 years. Press release; 2024. https://www.gla.ac.uk/news/archiveofnews/2024/february/headline_1049216_en.html
-
Gregg EW, Chen H, Bancks MP, Manalac R, Maruthur N, Munshi M, et al. Impact of remission from type 2 diabetes on long-term health outcomes: findings from the Look AHEAD study. Diabetologia. 2024;67(3):459-469. doi:10.1007/s00125-023-06048-6
-
Hamooya BM, Siame L, Muchaili L, Masenga SK, Kirabo A. Metabolic syndrome: epidemiology, mechanisms, and current therapeutic approaches. Frontiers in Nutrition. 2025;12. doi:10.3389/fnut.2025.1661603
-
Jahrami H, Trabelsi K, Husain W, Ammar A, BaHammam AS, Pandi-Perumal SR, et al. Prevalence of Orthosomnia in a General Population Sample: A Cross-Sectional Study. Brain Sciences. 2024;14(11):1123. doi:10.3390/brainsci14111123
-
Karabetian A, et al. The impact of exercise on chronic systemic inflammation: a systematic review and meta–meta-analysis. Sport Sci Health; 2025. https://link.springer.com/article/10.1007/s11332-025-01445-3
-
Ke J, Liu Q, Liu X, Wu K, Qiu H, Song J, et al. Prognostic value of C-reactive protein predicting all-cause and cause-specific mortality: a prospective cohort study in Shanghai, China. BMJ Open. 2025;15(8):e101532. doi:10.1136/bmjopen-2025-101532
-
Lean ME, Leslie WS, Barnes AC, Brosnahan N, Thom G, McCombie L, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. The Lancet. 2018;391(10120):541-551. doi:10.1016/S0140-6736(17)33102-1
-
Lee S, Tsai P, Yu K, Chan T. Effects of Mind–Body Interventions on Immune and Neuroendocrine Functions: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare. 2025;13(8):952. doi:10.3390/healthcare13080952
-
Greenway F, Loveridge B, Grimes RM, Tucker TR, Alexander M, Hepford SA, et al. Physiologic Insulin Resensitization as a Treatment Modality for Insulin Resistance Pathophysiology. International Journal of Molecular Sciences. 2022;23(3):1884. doi:10.3390/ijms23031884
-
Li M, Chi X, Wang Y, Setrerrahmane S, Xie W, Xu H. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduction and Targeted Therapy. 2022;7(1). doi:10.1038/s41392-022-01073-0
-
Li W, Chen D, Peng Y, Lu Z, Kwan M, Tse LA. Association Between Metabolic Syndrome and Mortality: Prospective Cohort Study. JMIR Public Health and Surveillance. 2023;9:e44073. doi:10.2196/44073
-
Liang R, Qi X, Cai Q, Niu L, Huang X, Zhang D, et al. The role of NLRP3 inflammasome in aging and age-related diseases. Immunity & Ageing. 2024;21(1). doi:10.1186/s12979-023-00395-z
-
Lim EL, Hollingsworth KG, Aribisala BS, Chen MJ, Mathers JC, Taylor R. Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia. 2011;54(10):2506-2514. doi:10.1007/s00125-011-2204-7
-
Liu S, Yang R, Zuo Y, Qiao C, Jiang W, Cheng W, et al. The association of circulating systemic inflammation with premature death and the protective role of the Mediterranean diet: a large prospective cohort study of UK biobank. BMC Public Health. 2024;24(1). doi:10.1186/s12889-024-18888-x
-
Liu Z, Lei M, Bai Y. Chronic Stress Mediates Inflammatory Cytokines Alterations and Its Role in Tumorigenesis. Journal of Inflammation Research. 2025;Volume 18:1067-1090. doi:10.2147/JIR.S485159
-
Margină D, Ungurianu A, Purdel C, Tsoukalas D, Sarandi E, Thanasoula M, et al. Chronic Inflammation in the Context of Everyday Life: Dietary Changes as Mitigating Factors. International Journal of Environmental Research and Public Health. 2020;17(11):4135. doi:10.3390/ijerph17114135
-
Mishra B, Agarwal A, George JA, Upadhyay AD, Nilima N, Mishra R, et al. Effectiveness of Yoga in Modulating Markers of Immunity and Inflammation: A Systematic Review and Meta-Analysis. Cureus. 2024. doi:10.7759/cureus.57541
-
Mishra S, Persons PA, Lorenzo AM, Chaliki SS, Bersoux S. Time-Restricted Eating and Its Metabolic Benefits. Journal of Clinical Medicine. 2023;12(22):7007. doi:10.3390/jcm12227007
-
Keshani M, Rafiee S, Heidari H, Rouhani MH, Sharma M, Bagherniya M. Mediterranean Diet Reduces Inflammation in Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Nutrition Reviews. 2025. doi:10.1093/nutrit/nuaf213
-
NIDDK. Insulin Resistance & Prediabetes. National Institute of Diabetes and Digestive and Kidney Diseases; 2024. https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/prediabetes-insulin-resistance
-
Papadaki A, Nolen-Doerr E, Mantzoros CS. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients. 2020;12(11):3342. doi:10.3390/nu12113342
-
Reynolds HR. High-Sensitivity C-Reactive Protein and Cardiovascular Risk. UpToDate; 2024. https://www.uptodate.com/contents/c-reactive-protein-in-cardiovascular-disease
-
Saavedra D, Añé-Kourí AL, Barzilai N, Caruso C, Cho K, Fontana L, et al. Aging and chronic inflammation: highlights from a multidisciplinary workshop. Immunity & Ageing. 2023;20(1). doi:10.1186/s12979-023-00352-w
-
Savulescu-Fiedler I, Mihalcea R, Dragosloveanu S, Scheau C, Baz RO, Caruntu A, et al. The Interplay between Obesity and Inflammation. Life. 2024;14(7):856. doi:10.3390/life14070856
-
Schnohr A, et al. Does Lifelong Exercise Counteract Low-Grade Inflammation Associated with Aging?. Sports Med.; 2025. https://link.springer.com/article/10.1007/s40279-024-02152-8
-
Shah VN, DuBose SN, Li Z, Beck RW, Peters AL, Weinstock RS, et al. Continuous Glucose Monitoring Profiles in Healthy Nondiabetic Participants: A Multicenter Prospective Study. The Journal of Clinical Endocrinology & Metabolism. 2019;104(10):4356-4364. doi:10.1210/jc.2018-02763
-
Silva FM, Duarte-Mendes P, Teixeira AM, Soares CM, Ferreira JP. The effects of combined exercise training on glucose metabolism and inflammatory markers in sedentary adults: a systematic review and meta-analysis. Scientific Reports. 2024;14(1). doi:10.1038/s41598-024-51832-y
-
Sofizadeh S, Pehrsson A, Ólafsdóttir AF, Lind M. Evaluation of Reference Metrics for Continuous Glucose Monitoring in Persons Without Diabetes and Prediabetes. Journal of Diabetes Science and Technology. 2020;16(2):373-382. doi:10.1177/1932296820965599
-
Suleiman M, Marselli L, Cnop M, Eizirik DL, De Luca C, Femia FR, et al. The Role of Beta Cell Recovery in Type 2 Diabetes Remission. International Journal of Molecular Sciences. 2022;23(13):7435. doi:10.3390/ijms23137435
-
Tabák AG, Jokela M, Akbaraly TN, Brunner EJ, Kivimäki M, Witte DR. Trajectories of glycaemia, insulin sensitivity, and insulin secretion before diagnosis of type 2 diabetes: an analysis from the Whitehall II study. The Lancet. 2009;373(9682):2215-2221. doi:10.1016/S0140-6736(09)60619-X
-
Tayebi SM, Poorhabibi H, Heidary D, Amini MA, Sadeghi A. Impact of aerobic exercise on chronic inflammation in older adults: a systematic review and meta-analysis. BMC Sports Science, Medicine and Rehabilitation. 2025;17(1). doi:10.1186/s13102-025-01279-z
-
Paul P, Kaul R, Harfouche M, Arabi M, Al-Najjar Y, Sarkar A, et al. The effect of microbiome-modulating probiotics, prebiotics and synbiotics on glucose homeostasis in type 2 diabetes: A systematic review, meta-analysis, and meta-regression of clinical trials. Pharmacological Research. 2022;185:106520. doi:10.1016/j.phrs.2022.106520
-
Wrona MV, Ghosh R, Coll K, Chun C, Yousefzadeh MJ. The 3 I’s of immunity and aging: immunosenescence, inflammaging, and immune resilience. Frontiers in Aging. 2024;5. doi:10.3389/fragi.2024.1490302
-
Xie W, Su F, Wang G, Peng Z, Xu Y, Zhang Y, et al. Glucose-lowering effect of berberine on type 2 diabetes: A systematic review and meta-analysis. Frontiers in Pharmacology. 2022;13. doi:10.3389/fphar.2022.1015045
-
Xin Y, Davies A, Briggs A, McCombie L, Messow CM, Grieve E, et al. Type 2 diabetes remission: 2 year within-trial and lifetime-horizon cost-effectiveness of the Diabetes Remission Clinical Trial (DiRECT)/Counterweight-Plus weight management programme. Diabetologia. 2020;63(10):2112-2122. doi:10.1007/s00125-020-05224-2
-
Yan L, Rust BM, Palmer DG. Time-restricted feeding restores metabolic flexibility in adult mice with excess adiposity. Frontiers in Nutrition. 2024;11. doi:10.3389/fnut.2024.1340735
-
Yang Y, Wang T, Xie H, Hu PP, Li P. Experimental cell models of insulin resistance: overview and appraisal. Frontiers in Endocrinology. 2024;15. doi:10.3389/fendo.2024.1469565
-
Yu YT, et al. Dietary glycemic index and insulin resistance in non-diabetic adults. Front Nutr; 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11864931/
-
Zuo L, Prather ER, Stetskiv M, Garrison DE, Meade JR, Peace TI, et al. Inflammaging and Oxidative Stress in Human Diseases: From Molecular Mechanisms to Novel Treatments. International Journal of Molecular Sciences. 2019;20(18):4472. doi:10.3390/ijms20184472