Unit 3: Advanced Topics & Disease Prevention¶
Chapter 3.18: Neuroprotection¶
[CHONK: 1-minute summary]
[CHONK: Brain Health Across the Lifespan]
Why brain health matters for longevity¶
When people think about living longer, they often imagine more years of physical capability: more hikes, more time with grandchildren, more independence.
But there's a fear that haunts many clients, often unspoken: What if my body outlasts my mind?
For most people, cognitive decline represents the worst-case aging scenario: losing the ability to recognize loved ones, forgetting precious memories, and losing independence in daily life. These fears run deep, and honestly? They're not unfounded. Dementia affects approximately 55 million people worldwide, with nearly 10 million new cases annually.
As a longevity coach, you'll encounter clients who want to discuss brain health but don't know how to bring it up. You'll work with people who've watched parents or grandparents decline cognitively and wonder if the same fate awaits them.
(This is emotionally heavy territory. It's okay if reading this brings up your own fears about aging. Most people have them.)
Understanding the science of neuroprotection, and the limits of what we can promise, will help you support these clients with both compassion and honesty. We can't guarantee prevention of cognitive decline. But substantial evidence suggests that lifestyle factors significantly influence brain health across the lifespan. Your role is to help clients take meaningful action on what's within their control, while maintaining realistic expectations.
The good news: modifiable risk factors¶
Now for the hopeful part. (And it's genuinely hopeful.)
The 2024 Lancet Commission on Dementia Prevention, a major international review of the evidence, concluded that addressing 14 modifiable risk factors could potentially prevent or delay approximately 45 percent of dementia cases worldwide. Let that sink in for a moment: not 5 percent or 10 percent, but nearly half.
These modifiable risk factors span the entire lifespan:
Early life:
- Lower educational attainment
Midlife:
- Hearing loss
- Traumatic brain injury
- Hypertension
- High LDL cholesterol (newly added in 2024)
- Excessive alcohol consumption
- Obesity
- Smoking
Later life and across the lifespan:
- Depression
- Social isolation
- Physical inactivity
- Diabetes
- Air pollution
- Untreated vision loss (newly added in 2024)
The 2024 update added two risk factors based on new evidence: high LDL cholesterol in midlife (accounting for approximately 7 percent of attributable risk) and untreated vision loss in later life (approximately 2 percent).
What these numbers mean¶
When researchers say 45 percent of dementia cases could be "prevented or delayed," they're using a concept called population attributable fraction: the proportion of cases that might not occur if these risk factors were eliminated. This is a theoretical maximum based on current evidence, assuming the relationships are causal.
Important caveats:
- These are observational associations; causality isn't definitively proven for all factors
- A 2023 study using genetic analysis (Mendelian randomization) found limited genetic evidence supporting causal effects for some risk factors, suggesting some associations may reflect confounding
- Risk factors overlap and interact. You can't simply add the percentages together
- Individual risk reduction will vary based on genetics, other factors, and timing of intervention
- Still, even if the true preventable proportion is lower, the evidence strongly suggests that lifestyle choices matter for brain health, and that's something coaches can work with.
If all those percentages and caveats feel a bit abstract, that's OK. The key takeaway is that everyday habits really do matter for brain health, even if we can't pin down an exact number for any one person.
What we can and can't promise¶
No lifestyle intervention has been proven in randomized trials to definitively prevent dementia. The evidence for modifiable risk factors comes primarily from observational studies. People who exercise more, eat healthier, stay socially connected, and manage cardiovascular risk tend to have lower rates of cognitive decline and dementia.
Does this mean exercise causes better brain health, or that healthier people are simply more likely to exercise? We can't be certain from observational data alone. The relationships are likely bidirectional and influenced by many factors.
What we CAN say to clients:
- "The evidence suggests that these lifestyle factors are associated with better cognitive outcomes"
- "We can focus on reducing modifiable risk factors"
- "These interventions benefit your overall health regardless of brain-specific effects"
- "We're optimizing what's within your control"
What we should NOT say:
- "This will prevent Alzheimer's"
- "Following this program guarantees you won't get dementia"
- "If you do everything right, you're protected"
- The reframe: We optimize, we don't guarantee. And fortunately, everything that supports brain health also supports overall health, so there's no downside to focusing on these factors.
Cognitive reserve: building your brain's buffer¶
One of the most hopeful concepts in brain health research is cognitive reserve: the brain's ability to improvise and find alternate ways of completing a task when faced with damage or age-related changes.
Think of it like having multiple routes to the same destination. If one road is blocked, you can take another. People with higher cognitive reserve have more "alternate routes," more neural pathways and connections that can compensate when some are damaged.
Research suggests cognitive reserve is built through:
- Education and lifelong learning: Not just formal schooling, but continued intellectual engagement
- Occupational complexity: Jobs that involve complex thinking, problem-solving, and learning
- Social engagement: Rich social networks and meaningful relationships
- Physical activity: Exercise that challenges both body and mind
- Novel experiences: Learning new skills, traveling, encountering new ideas
The concept of cognitive reserve helps explain why some people with significant brain pathology (visible on autopsy) maintained normal cognitive function during life, while others with less pathology showed dementia symptoms. The difference appears to be the "buffer" built through a lifetime of cognitive engagement.
For coaching, this means: it's never too late to build cognitive reserve. Even in late life, engaging in new learning, social connection, and physical activity may strengthen this buffer.
| For DIY Learners |
|---|
| Applying this to yourself: When was the last time you learned something genuinely new, not just consumed content, but developed a skill that challenged your brain? Learning a musical instrument, studying a language, picking up a new sport, or diving into an unfamiliar subject all build cognitive reserve. It doesn't have to be dramatic. Even small cognitive challenges (a new recipe, a different route to work, a book outside your usual genre) contribute. The discomfort of not-knowing is actually the feeling of building new neural pathways. |
The metabolic-cognitive connection¶
As you learned in Chapter 17 on metabolic health, what happens in the body profoundly affects the brain. This is particularly true for metabolic dysfunction.
The brain:
- Uses approximately 20 percent of the body's energy despite being only 2 percent of body weight
- Requires a constant supply of glucose and oxygen
- Is exquisitely sensitive to insulin signaling
- Is vulnerable to vascular damage from hypertension and dyslipidemia
Insulin resistance, the metabolic dysfunction underlying Type 2 diabetes, doesn't just affect blood sugar. It affects the brain's ability to use glucose efficiently, increases inflammation, and may contribute to the accumulation of abnormal proteins associated with Alzheimer's disease.
This connection is so strong that some researchers have called Alzheimer's "Type 3 diabetes," though this remains controversial and oversimplifies a complex disease. What's clear is that metabolic health and brain health are deeply intertwined, and interventions that improve one often improve the other.
[CHONK: The Science of Neuroprotection]
Understanding brain health mechanisms¶
To support clients in their brain health work, you need a basic understanding of the mechanisms involved, not to diagnose or treat, but to explain why certain interventions might help and to answer common questions.
BDNF: Miracle-Gro for the brain¶
You encountered BDNF (brain-derived neurotrophic factor) in Chapter 2.9 when we discussed how exercise benefits the brain. A quick refresher with a bit more context will help here.
BDNF is a protein that acts like fertilizer for neurons (brain cells). It:
- Supports the survival of existing neurons
- Encourages the growth of new neurons (neurogenesis), particularly in the hippocampus (the brain's memory center)
- Promotes the formation of new connections between neurons (synapses)
- Helps with learning and memory consolidation
BDNF levels naturally decline with age, and lower levels are associated with depression, cognitive decline, and neurodegenerative diseases. The good news: certain lifestyle factors can boost BDNF production.
What increases BDNF:
- Exercise (particularly aerobic and resistance training)
- Learning new skills
- Social engagement
- Certain dietary patterns (especially those rich in flavonoids and omega-3 fatty acids)
- Quality sleep
What decreases BDNF:
- Chronic stress
- Sedentary behavior
- Inflammatory diet
- Social isolation
- Poor sleep
Meta-analyses confirm that exercise reliably increases peripheral (blood) BDNF levels, with moderate-intensity resistance training showing particularly large effects in some studies. Functional training (exercise that mimics real-world movements) may produce larger BDNF increases than isolated aerobic exercise alone.
The glymphatic system: your brain's overnight cleanup crew¶
As you learned in Chapter 2.11 on sleep optimization, the brain has its own waste clearance system called the glymphatic system. This system is most active during sleep, particularly during deep (slow-wave) sleep.
Rather than repeating that material, focus on what's important for neuroprotection:
The glymphatic system clears metabolic waste from the brain, including amyloid-beta, a protein that accumulates in Alzheimer's disease. Poor sleep disrupts this clearance process, potentially allowing harmful substances to accumulate.
Key point for clients: Sleep isn't just rest. It's when your brain takes out the trash. Chronic sleep deprivation doesn't just leave you tired, it may allow waste products to build up in brain tissue.
For more detail on the glymphatic system and sleep optimization strategies, refer clients and yourself back to Chapter 2.11.
Inflammation and the brain¶
Chronic low-grade inflammation (the type associated with obesity, metabolic dysfunction, poor diet, chronic stress, and sedentary behavior) affects the brain in multiple ways:
- Crosses the blood-brain barrier and activates brain immune cells (microglia)
- Disrupts normal neuronal function
- May contribute to the formation of abnormal protein deposits
- Impairs BDNF signaling
- Damages blood vessels that supply the brain
This is why interventions targeting inflammation (anti-inflammatory diets, exercise, stress management, quality sleep) may benefit brain health even if they don't directly target the brain itself.
The vascular hypothesis: heart health is brain health¶
The brain depends entirely on blood vessels to deliver oxygen and nutrients. Anything that damages blood vessels (hypertension, high cholesterol, diabetes, smoking) damages the brain.
This vascular connection explains why:
- Cardiovascular disease and dementia share many risk factors
- Mid-life hypertension is a significant dementia risk factor
- High LDL cholesterol in midlife (newly recognized in 2024) increases dementia risk
- Stroke can cause vascular dementia directly
The practical implication: Much of what we do to protect the heart also protects the brain. Cardiovascular risk management isn't separate from brain health. It IS brain health.
A brief word on Alzheimer's pathophysiology¶
You may wonder about amyloid plaques and tau tangles, the abnormal protein deposits found in Alzheimer's disease. For coaches, the key points are:
Alzheimer's disease is characterized by:
- Accumulation of amyloid-beta protein into plaques outside neurons
- Accumulation of tau protein into tangles inside neurons
- Progressive loss of synapses and neurons
However, these pathological changes can begin 20+ years before symptoms appear, and some people accumulate significant pathology without ever developing dementia (this is where cognitive reserve comes in).
Current drug treatments targeting amyloid have shown modest effects at best, and the field is moving toward earlier intervention and multifactorial approaches, which aligns perfectly with the lifestyle-focused prevention strategies we'll discuss.
What coaches don't need to know: The detailed molecular mechanisms, genetic testing interpretation, or treatment protocols. Leave that to neurologists and geriatricians. Focus on what clients can actually do.
Coaching in practice: Explaining brain science accessibly¶
When clients ask about brain mechanisms, your goal is to keep things simple, accurate, and reassuring.
What NOT to do:
❌ Launch into a long lecture about BDNF, glymphatic flow, and neurodegeneration.
Why it doesn't work: Most clients just want a clear picture, not a mini biology class.
What TO do:
✅ Use short, everyday metaphors and check that your explanation lands.
Client: Why does exercise actually help my brain?
Coach: Great question. When you move your body, you make more of a protein called BDNF. You can think of it like fertilizer for brain cells, it helps them stay healthy and grow new connections, especially in memory areas. Does that picture make sense?
Client: Yeah, that helps. Fertilizer for my brain, I can remember that.
Client: What about sleep? Why is that so important for my brain?
Coach: While you sleep, your brain turns on a cleanup system that clears out waste products. It's like having a night crew that comes in to clean an office, but they can only work when everyone goes home. If you don't get enough sleep, the trash piles up.
Client: And inflammation? Does that really affect my brain too?
Coach: Yes. Chronic inflammation can cross into the brain and disrupt normal function. The good news is that many things that reduce inflammation in the body, like good food, regular movement, sleep, and stress management, also protect the brain.
[CHONK: Evidence-Based Brain Health Strategies]
What actually works for brain health¶
Brain health advice can get noisy fast, especially once you add scary headlines and flashy supplement marketing. Here, you’ll see specific interventions, how strong the evidence is for each one, and how to turn that into real coaching decisions. We’ll also be clear about what the research supports and where there’s still uncertainty. That’s normal in this field.
Exercise: the #1 brain health intervention¶
Evidence level: Strong (for association and cognitive benefits in those with impairment); Moderate-to-Strong (for prevention in healthy adults)
If you could only recommend one thing for brain health, it would be exercise, because the evidence is strong across multiple lines of research. Good news: it’s accessible, and it works.
What the research shows:
For cognitive function:
- Meta-analyses consistently show that exercise improves cognitive function, particularly in older adults with existing cognitive impairment
- A 2025 umbrella review in the British Journal of Sports Medicine concluded there's strong evidence that exercise, even at light intensity, benefits cognition, memory, and executive function across populations
- Combined aerobic and resistance training shows a pooled effect size (Hedges' g) of approximately 0.32 for cognitive improvement, a small-to-moderate effect
For dementia risk:
- The highest levels of physical activity are associated with 26-40 percent lower dementia risk compared to the least active
- A dose-response relationship exists: every 10 MET-hours per week of additional activity is associated with approximately 15 percent lower Alzheimer's risk
- One large UK Biobank analysis found that dementia risk reduction became significant only above 300 minutes per week of moderate-to-vigorous activity
If all those percentages and effect sizes start to blur together, you’re not alone. The simple coaching takeaway is: move more, build consistency, and if a client wants to optimize, gradually work toward higher weekly volume. You don’t have to “biohack” this.
Dose and type:
The evidence suggests:
| Parameter | Recommendation | Evidence |
|---|---|---|
| Minimum effective dose | 150 minutes/week moderate activity | Associated with some benefit |
| Optimal for brain health | 300+ minutes/week moderate activity, or equivalent | Larger risk reduction seen at higher doses |
| Type | Combined aerobic + resistance | Most consistent benefits (effect size ≈0.32) |
| Intensity | Vigorous activity may contribute disproportionately | UK Biobank: vigorous activity contributed ~79% of protective effect |
Dual-task activities:
One especially interesting category for brain health is “dual-task” activities: physical exercise combined with cognitive challenges.
- Walking while having a conversation (or doing a “walking meeting”)
- Dance classes and sports that make you learn sequences, react, and strategize while you move
- Exercise video games ("exergaming")
Multiple studies show dual-task training produces greater cognitive improvements than single-task exercise alone, particularly for executive function and daily functioning.
| For DIY Learners |
|---|
| Applying this to yourself: Your brain health is built daily through the same fundamentals we've covered throughout this course: exercise (especially combined cardio + strength), sleep, nutrition, stress management, and social connection. If you’re worried about cognitive decline, it can be tempting to reach for nootropic supplements. That’s understandable. But the better first move is usually something like a walk with a friend, a challenging new skill to learn, and 7+ hours of sleep. These have far better evidence than any brain-boosting pill. |
Practical application for coaching:
- Any movement is better than none, so don’t let perfect be the enemy of good
- Build toward 300+ minutes/week for clients motivated to optimize brain health
- Include both aerobic and resistance training when possible
- Incorporate dual-task elements: walking meetings, dance classes, sports with strategic components
- Vigorous exercise may offer additional benefits, but only if clients can do it safely
Coaching in practice: The client who thinks exercise “won’t matter”
What NOT to do:
❌ Lead with the minute targets, MET-hours, and effect sizes.
What TO do:
Client: I’m not an “exercise person,” and I’m wondering if it’ll really make a difference.
Coach: I hear you, and yes, it can. Would you be open to starting with something small, like two 10-minute walks this week?
Client: Yeah, I could do that.
Coach: Great. We’ll build from there. Consistency matters most, and if you decide you want to optimize later, we can gradually work toward more weekly movement and add some strength work.
Nutrition: the MIND diet and beyond¶
Evidence level: Moderate (strong observational data, mixed RCT results)
The MIND diet (Mediterranean-DASH Intervention for Neurodegenerative Delay) was designed specifically with brain health in mind, combining elements of the Mediterranean and DASH diets with foods that show up repeatedly in cognition research.
Core components of the MIND diet:
Emphasized foods:
- Vegetables: green leafy vegetables (at least 6 servings/week) and other vegetables (at least 1 serving/day)
- Berries, especially blueberries (at least 2 servings/week)
- Nuts (at least 5 servings/week) and beans (at least 4 servings/week)
- Whole grains (at least 3 servings/day)
- Fish (at least 1 serving/week) and poultry (at least 2 servings/week)
- Olive oil as primary cooking oil
- Wine (1 glass/day, optional and controversial)
Limited foods:
- Red meat (less than 4 servings/week) and cheese (less than 1 serving/week)
- Butter/margarine (less than 1 tablespoon/day)
- Pastries/sweets (less than 5 servings/week) and fried/fast food (less than 1 serving/week)
What the research shows:
Observational studies:
- Higher MIND diet adherence is consistently associated with slower cognitive decline and lower dementia risk
- The original MIND diet research found that those with the highest adherence showed approximately 53 percent slower cognitive decline compared to those with the lowest adherence
- A meta-analysis of seven cohorts (n=26,103) found each 1 standard deviation increase in MIND score predicted 0.042 units higher global cognition
- One large study (JAMA Psychiatry 2023) found highest adherence associated with approximately 17 percent lower incident dementia risk
Randomized controlled trials:
- A 3-year RCT published in the New England Journal of Medicine (2023) found no significant cognitive difference between MIND diet and control diet groups
- However, both groups in this trial improved their diets, potentially diluting the effect
- Multidomain trials that include MIND diet plus other interventions (like the U.S. POINTER trial) show more promising results
Putting the evidence together:
The MIND diet appears beneficial based on observational data, but the only dedicated RCT showed null results over 3 years. This doesn't mean the diet doesn't work; it may mean:
- Effects take longer than 3 years to manifest
- Diet-alone interventions are insufficient; multidomain approaches may be needed
- The comparison group also improved their diet, reducing the contrast.
That mix of “promising but not definitive” can feel frustrating. Coaches (and clients) often wish the science were cleaner, but learning how to make good decisions with imperfect evidence is part of being an effective longevity coach.
Practical application:
Rather than rigidly prescribing the MIND diet, focus on the key principles:
1. Aim for more vegetables, especially leafy greens, and keep it practical for the client’s routine
2. Add berries regularly, particularly blueberries, which are rich in brain-protective flavonoids
3. Include fatty fish when possible as a top food source of omega-3 fatty acids (see supplements section)
4. Build meals around nuts, olive oil, beans, and whole grains to match a Mediterranean-style eating pattern
5. Pull back on ultra-processed foods like fried foods and added sugars, which tend to crowd out more protective choices
Coaching in practice: The client who wants a strict MIND “rulebook”
What NOT to do:
❌ Hand over a rigid food list and treat it like an all-or-nothing pass/fail test.
What TO do:
Client: Do I need to follow the MIND diet perfectly for it to count?
Coach: No. We can focus on the highest-impact pieces first. Which feels like the easiest starting point for you: adding a couple servings of vegetables most days, or adding berries a few times a week?
Sleep: when your brain cleans house¶
Evidence level: Moderate-to-Strong
Sleep’s importance for brain health is covered extensively in Chapter 2.11. Here are the key points most relevant to neuroprotection, plus where a coach can really help. You don’t have to “optimize” sleep. You just have to take it seriously.
- The glymphatic system clears brain waste most effectively during deep sleep
- Chronic short sleep (less than 7 hours) is associated with increased dementia risk
- Sleep disorders like obstructive sleep apnea are risk factors for cognitive decline
- Sleep consolidates memories and supports neuroplasticity
Coach's role:
- Screen for sleep concerns with a few basic questions, then support sleep hygiene improvements (Chapter 2.11)
- When you suspect a sleep disorder, refer to medical evaluation (for example, suspected obstructive sleep apnea)
Coaching in practice: The client who might have sleep apnea
What NOT to do:
❌ Diagnose sleep apnea, or tell them to “just sleep more.”
What TO do:
Client: My partner says I snore, and I still wake up exhausted.
Coach: Thanks for telling me. I can’t diagnose anything, but those can be signs of sleep apnea. Would you be willing to talk with your doctor about a sleep evaluation? In the meantime, we can work on a few sleep-hygiene basics.
Social connection and purpose¶
Evidence level: Moderate (consistent observational data, limited intervention trials)
One of the most important, and most often missed, brain health factors is social connection. Not because people are “doing it wrong,” but because connection is harder to schedule than a workout.
What the research shows:
Social isolation and dementia risk:
- The largest meta-analysis to date (n=608,561) found loneliness increases all-cause dementia risk by approximately 31 percent
- Alzheimer's disease risk increased by 39 percent, and vascular dementia risk by 74 percent
- Social isolation (objectively measured) is associated with approximately 28 percent higher hazard of dementia over 9 years
- Even "digital isolation", limited internet/electronic communication, is associated with 36 percent higher dementia risk
Purpose in life:
- Higher purpose in life is associated with lower likelihood of dementia (odds ratio approximately 0.85)
- Purpose appears to provide resilience against cognitive decline even in the presence of brain pathology
- A 28-year prospective study found higher purpose at midlife predicts better cognition in later life
Mechanisms:
Social connection likely protects cognition through multiple pathways:
- More cognitive stimulation through conversation and shared activities
- Lower stress load via social support (which can reduce cortisol and stress responses)
- Neurochemical and neurotrophic effects, including higher BDNF and oxytocin with positive social interactions
- Lower depression risk (a dementia risk factor)
Practical application:
- Assess social connection as part of Deep Health evaluation
- Help clients identify opportunities for meaningful social engagement
- Support purpose clarification: what gives their life meaning?
- Watch for isolation as a warning sign, especially in retirement, widowhood, or relocation
- Consider group-based interventions when available (walking groups, classes, volunteer work)
A quick way to bring this to life in coaching:
Client: I’m too busy for social stuff right now.
Coach: That makes sense. When life gets full, connection is usually the first thing to slide. What’s one small, realistic move this week, like a 10-minute call or a walk with someone you like?
Why prioritizing social connection is hard¶
The uncomfortable truth is that social connection is one of the most powerful brain-protective interventions we have, yet it’s often the first thing to get squeezed out when life gets busy.
For many clients, it’s easier to add a supplement than to call an old friend, and it’s more convenient to buy a brain-training app than to join a community group. Solitary interventions can feel more controllable and more “efficient,” especially when someone is tired, stressed, or anxious.
But the research is clear: loneliness increases dementia risk by 31%, which isn’t a small effect. So when a client says they’re “too busy” for social connection, the goal isn’t to guilt them. It’s to help them see that this isn’t optional self-care. It’s a foundational brain health intervention, as important as exercise, and maybe more so.
| For DIY Learners |
|---|
| Applying this to yourself: Be honest: how connected do you actually feel? Not how many people you know, but how many people you could call if you were having a hard day. How many conversations have you had this week where you felt genuinely seen and understood? If the answers make you uncomfortable, that’s information. Social connection isn’t a nice-to-have. The effect sizes for loneliness and dementia are comparable to major physical risk factors. What’s one small step you could take this week to deepen a connection? |
Coaching in practice: The client who dismisses social connection¶
You’ll likely hear some version of this: "I'm an introvert. I don't need other people."
What NOT to do:
❌ Jump in with a lecture about studies on loneliness and dementia risk.
Why it doesn't work: Clients can feel judged or pressured, and it reinforces the idea that connection only "counts" if it looks a certain way.
What TO do:
✅ Validate their temperament and explore what meaningful connection could look like for them.
Client: I'm an introvert. I don't need other people.
Coach: That makes sense. Social health doesn't mean being the life of the party or having a huge circle of friends. It’s usually more about a few relationships that feel meaningful and supportive. When you think about your life right now, which relationships feel most important to you?
Client: Probably my sister, and one friend from work.
Coach: Great. We can work with that, and we can keep it comfortable for you. Quality matters more than quantity. How might you nurture those relationships in ways that fit your personality?
Cognitive stimulation and lifelong learning¶
Evidence level: Moderate for cognitive benefits; Limited for far-transfer to real-world function
"Use it or lose it" has some truth, but the details matter. In practice, it helps to separate what improves test performance from what actually carries over into day-to-day life. It’s easy to mix up, especially with slick marketing.
What the research shows:
Cognitive training:
- Working memory training reliably improves performance on trained tasks (effect size approximately 0.34)
- However, far-transfer, improvement in untrained tasks and real-world function, is generally small or absent
- Commercial "brain games" (like Lumosity) show little evidence of real-world cognitive benefits
- Training with everyday, functional cognitive tasks shows better transfer than abstract brain games
Novel learning:
- Learning new skills, particularly complex skills involving multiple domains, appears more beneficial than repetitive "brain exercises"
- Activities that combine cognitive, physical, and social elements (like dance classes, learning an instrument, or group language learning) may offer multiple benefits
What this means in practice:
Brain games are unlikely to protect against dementia, despite marketing claims. The FTC actually sued Lumosity for deceptive advertising. However, staying cognitively engaged, especially through novel, meaningful activities, appears to help maintain cognitive function.
Practical application:
Instead of prescribing brain games, encourage:
1. Learning new skills: language, music, art, crafts
2. Activities combining multiple elements: dance (physical + cognitive + social), group classes, sports with strategic components
3. Reading and engaging with complex material
4. Meaningful hobbies that challenge thinking
5. Educational pursuits at any age
What NOT to do:
❌ Treat an app like a “prescription” for dementia prevention.
What TO do:
Client: “Should I use a brain-training app?”
Coach: “If you enjoy it, it’s fine as entertainment. But if your goal is brain health, learning a new language or instrument is more likely to help, and it’s usually a lot more meaningful.”
Supplements for brain health¶
Evidence level: Modest for omega-3s; Preliminary for creatine
Clients frequently ask about supplements for brain health, and it makes sense. Supplements can feel like an easy “add-on.” The research, though, paints a more modest picture than many headlines suggest, so setting expectations upfront really helps.
Coaching in practice: The client who wants a supplement plan
What NOT to do:
❌ Promise big cognitive gains, or imply supplements can replace sleep, exercise, and an overall healthy diet pattern.
What TO do:
Client: I just want to take something for brain health. What should I use?
Coach: We can talk options. Before we do, can I ask how sleep and exercise are going? Those are still the biggest levers for brain health. If you want an add-on after that, omega-3s have modest evidence, and we can set realistic expectations.
Omega-3 fatty acids (DHA/EPA):
What the research shows:
- Umbrella reviews of trials show a small but statistically significant improvement in global cognition (effect size approximately 0.16) with EPA+DHA supplementation in older adults without dementia
- Observational data consistently links higher omega-3 intake with lower dementia risk. One analysis found long-term supplement use associated with 64 percent lower Alzheimer's risk
- Effects appear more pronounced for executive function and at doses around 500-2000 mg/day
- Benefits may depend on baseline omega-3 status and genetics (APOE status)
Practical recommendation:
- Encourage fatty fish consumption (2+ servings/week)
- If supplementing, 500-2000 mg combined EPA+DHA is the range studied
- Set realistic expectations: effects are modest, not dramatic
- Priority should remain on foundational interventions (exercise, sleep, diet pattern)
Creatine:
What the research shows:
- Meta-analyses show small improvements in memory (effect size approximately 0.31) and attention/processing speed
- Benefits appear more pronounced in older adults, vegetarians, or during conditions of energy stress (like sleep deprivation)
- Large RCTs in healthy young adults show little to no effect
- The European Food Safety Authority (2024) concluded that a cause-effect relationship between creatine and improved cognition has not been established
Practical recommendation:
- Not a first-line recommendation for brain health
- May have modest benefits for older adults or those under energy stress
- Standard dose in studies: 3-5 grams/day
- Generally safe with mild GI side effects in some people
For deeper supplement discussion, refer to Chapter 15 on Supplements for Longevity.
Heat therapy and sauna¶
Evidence level: Preliminary (observational data only, limited generalizability)
The longevity protocol mentions sauna use for dementia risk reduction. The data so far are intriguing, and it’s also a great example of why we have to keep our “evidence goggles” on: association isn’t causation.
What the research shows:
- Finnish cohort studies found men who used sauna 4-7 times/week had approximately 66 percent lower dementia risk compared to once-weekly users
- A second Finnish study found 9-12 sauna sessions/month associated with about 50 percent lower risk over the first 20 years of follow-up
- Plausible mechanisms include improved cardiovascular function, heat shock protein activation, and relaxation effects
Critical caveats:
- All evidence is observational and from Finnish populations with specific sauna traditions
- Causality is not established; frequent sauna users may differ in many ways from infrequent users
- Effects may not generalize to other populations or sauna types
- No randomized trials have tested sauna for cognitive outcomes
If you’re unsure how excited to be about sauna after hearing all of that, that’s appropriate. You can be transparent with clients that the data are interesting but still early, and keep sauna in the “optional extra” category.
Practical recommendation:
- If clients enjoy sauna and have access, it may be a reasonable addition to their wellness routine
- 2-4 sessions weekly at traditional Finnish temperatures (80-100°C/176-212°F) is the range associated with benefits
- Ensure adequate hydration and appropriate precautions
- Do NOT present this as essential or proven for dementia prevention
- This is "nice-to-have, not need-to-have"
[CHONK: The Modifiable Risk Factors]
The Lancet Commission's 14 factors¶
The 2024 Lancet Commission on Dementia Prevention provides the most thorough overview of modifiable risk factors. Below, we’ll go factor by factor, focusing on what the research suggests and how you can translate that into practical coaching.
What matters most is how you help a real person make a real change, not memorizing percentages.
Early life¶
Lower educational attainment (~5% of attributable risk)
This one can feel uncomfortable. After all, what can someone do about past access to education? A helpful reframe is that this factor reflects how early cognitive stimulation and learning help build cognitive reserve, and the brain keeps adapting throughout life.
For coaching, this means:
- You can’t change the past, but you can help clients build cognitive reserve now through ongoing learning and new challenges
- Encourage educational pursuits at any age, because the brain doesn’t stop benefiting from learning, including later in life
- If clients have children or grandchildren, support educational engagement and curiosity at home, not just “school performance”
Midlife¶
Hearing loss (~7% of attributable risk)
Hearing loss is one of the largest modifiable risk factors. The likely mechanisms include reduced cognitive stimulation and increased social isolation when hearing is impaired, which can quietly change how often someone engages with the world.
Coaching implications:
- Encourage hearing screening for clients over 50, especially if family members are noticing changes
- Support hearing aid use if recommended, and normalize any hesitation
- Connect the dots between untreated hearing loss and social withdrawal, so clients understand why this matters beyond “hearing better”
Traumatic brain injury
Even “mild” concussions, especially repeated ones, increase dementia risk. For coaches, that often means looking for history and patterns, not diagnosing anything.
For coaches:
- Ask about head injury history, including sports, falls, and work-related injuries
- Support appropriate protective equipment for higher-risk activities (helmets, safer setups, and smarter training choices)
- Refer clients with concussion history who notice cognitive changes, so they can be assessed by the right clinician
Hypertension
High blood pressure in midlife damages brain blood vessels over time, which means brain health and cardiovascular health are tightly linked.
Coaching approach:
- Encourage blood pressure monitoring (home cuffs can make this easier and more consistent)
- Support lifestyle interventions like exercise, weight management, sodium reduction, and stress management
- Emphasize the brain-health connection so it’s not framed as “just avoiding heart attacks”
High LDL cholesterol (~7% of attributable risk, newly added in 2024)
Midlife LDL appears to affect brain health through vascular mechanisms and possibly direct effects on amyloid pathways.
Coaching implications:
- Treat cardiovascular risk management as brain health management (because that’s what it is)
- Support Mediterranean-style eating patterns as a practical, food-first strategy
- Encourage regular lipid screening and conversations with healthcare providers, especially when numbers are trending up
Excessive alcohol
Heavy drinking can damage the brain directly and indirectly (through liver damage, nutritional deficiencies, and falls). The definition of “excessive” varies, but generally:
- More than 14 drinks/week is associated with brain harm
- Even moderate drinking may not be protective, despite earlier claims
- Support clients who want to reduce alcohol consumption by working on realistic, stepwise changes (cutting back can be a big deal for people)
Obesity
Midlife obesity increases dementia risk through multiple pathways, including inflammation, insulin resistance, vascular damage, and sleep apnea. At the same time, this topic needs careful handling because the weight–dementia relationship isn’t straightforward.
However:
- The relationship is complex, since late-life weight loss may actually be a dementia sign rather than a protective factor
- Keep the focus on metabolic health (Chapter 17) rather than just body weight, which tends to lead to better coaching conversations anyway
Smoking
Smoking damages brain blood vessels and increases inflammation and oxidative stress, so any move toward quitting supports brain health.
For coaches:
- Support smoking cessation without judgment (shame rarely helps people change)
- Reinforce that any reduction helps, especially as a stepping stone toward quitting
- Consider referral to cessation programs when extra support would make success more likely
Later life and across the lifespan¶
Depression
Depression both increases dementia risk and can be an early symptom of cognitive decline, so the relationship goes both ways.
The relationship is bidirectional:
- Chronic depression may affect the brain through stress hormones and inflammation, and early dementia may also manifest as depression
- Treatment of depression may reduce dementia risk, though this isn’t proven
Coaching role: screen for depression, support mental health help-seeking, and never try to treat depression yourself. If that boundary feels a little strict, that’s because it’s there to protect your client and you. (You’re still helping by getting them to the right support.)
Social isolation (~5% of attributable risk)
As discussed earlier, social disconnection significantly increases dementia risk, and it often sneaks in during stressful seasons of life.
Coaching approaches:
- Assess social connection as part of routine check-ins, the same way you’d ask about sleep or movement
- Help problem-solve barriers to social engagement (time, transportation, anxiety, hearing/vision issues)
- Consider group-based interventions when possible, since structure can make connection easier
- Watch for isolation during major life transitions like retirement, widowhood, or relocation
Physical inactivity
Covered extensively in the exercise section, but here’s the key point: for most clients, this is likely the most actionable factor, and small increases in movement can add up fast.
Diabetes
Diabetes increases dementia risk through multiple mechanisms, including vascular damage, insulin resistance in the brain, and inflammation.
For coaches:
- Support diabetes prevention through lifestyle (Chapter 17)
- Help clients with diabetes improve glycemic control through lifestyle factors, in collaboration with their healthcare team
- Keep reinforcing the big idea that diabetes management is brain health management
Air pollution
This is harder for individuals to control, but coaches can still help clients make meaningful moves where they can. (Even small improvements can matter.)
Coaches can:
- Encourage indoor air quality improvements like air filters and houseplants
- Support policy awareness and advocacy if clients are interested
- Suggest timing outdoor exercise to avoid high-pollution periods in affected areas
Untreated vision loss (~2% of attributable risk, newly added in 2024)
Vision loss in later life is associated with approximately 47 percent higher dementia risk. Cataract surgery is associated with 29 percent reduced dementia incidence.
For coaches:
- Encourage regular eye exams, particularly as clients age
- Support addressing vision problems promptly, since delays can increase isolation and reduce activity
- Explain that vision loss, like hearing loss, can reduce cognitive stimulation and social engagement
A note on genetics¶
Clients often ask about genetic risk, particularly the APOE gene. That question makes sense, and it often comes with a lot of emotion attached. Here's what coaches need to know.
APOE basics:
- APOE comes in three variants: ε2, ε3, and ε4
- APOE ε4 is associated with increased Alzheimer’s risk (about 2-3x higher with one copy, 8-12x higher with two copies)
- However, APOE ε4 is neither necessary nor sufficient for Alzheimer’s. Many ε4 carriers never develop dementia, and many without ε4 do
The coaching message:
- Genetics load the gun; lifestyle may pull or not pull the trigger
- Modifiable risk factors matter for everyone, regardless of genetics
- Some evidence suggests lifestyle interventions may be particularly important for those with genetic risk
- Genetic testing interpretation is outside coaching scope. Refer to genetic counselors if clients want testing (and if they’re feeling anxious about results, that’s completely normal)
For clients interested in genetics and nutrition, Precision Nutrition has a detailed e-book on genetic testing available at: https://www.precisionnutrition.com/genetic-testing-ebook
Coaching conversations: bringing the factors to life¶
What NOT to do (a well-meaning lecture):
Coach: “You need to get a hearing aid, start checking your blood pressure every day, cut out salt, quit smoking, fix your A1c, and avoid air pollution. These are the risk factors.”
Try this instead (short, real conversations):
Hearing loss
Client: “My partner says I keep turning the TV up.”
Coach: “That’s a useful clue. Would you be open to booking a hearing screen? If anything is recommended, we can talk through what would make it easier to follow through.”
Early life (education / learning)
Client: “I didn’t finish school. Does that mean I’m doomed?”
Coach: “No. This factor is more about cognitive stimulation over time. What’s one thing you’d actually enjoy learning this month, like a class, a hobby, or even a daily puzzle routine?”
Traumatic brain injury
Client: “I had a few concussions playing soccer.”
Coach: “Thanks for telling me. I’m not here to diagnose, but I do want to understand your history and how you’re feeling now. Have you noticed headaches, brain fog, or memory changes? If so, let’s loop in your clinician, and we can also talk about ways to lower risk going forward.”
Hypertension / cholesterol
Client: “My numbers are trending up, but I don’t feel any different.”
Coach: “Totally common. Would it help to track your blood pressure at home for two weeks so we can spot patterns? Then we can choose one lever to start with, like a short daily walk or a couple of lower-sodium swaps.”
Excessive alcohol
Client: “I drink most nights, and I’d like to cut back.”
Coach: “Okay. What would feel realistic this week, like two alcohol-free nights, smaller pours, or swapping one drink for something else you enjoy? We’ll pick one and make it easy to repeat.”
Obesity / metabolic health
Client: “My doctor told me to lose weight for my brain. I hate that conversation.”
Coach: “That makes sense. Instead of fixating on the scale, can we focus on the habits that improve metabolic health, like sleep, daily movement, and more balanced meals? Those changes support brain health either way.”
Smoking
Client: “I know I should quit. I’m just not there yet.”
Coach: “Thanks for being straight about it. What feels doable right now: cutting down, changing when you smoke, or getting extra support through a cessation program? We can take this one step at a time.”
Diabetes
Client: “My doctor says my A1c is high, and I’m overwhelmed.”
Coach: “I hear you. What did your care team recommend, and what part feels hardest to implement? We can focus on one change this week, like after-meal walks or a more balanced breakfast, and keep your clinician in the loop.”
Air pollution
Client: “Outdoor workouts help my stress, but the air quality is rough where I live.”
Coach: “Let’s work with what you can control. On high-pollution days, would an indoor option or a different time of day work? And at home, would you consider an air filter in the bedroom?”
Vision loss
Client: “I’ve stopped driving at night. It’s starting to limit me.”
Coach: “That makes sense. When’s your next eye exam? If it’s been a while, let’s get that scheduled, and in the meantime we can brainstorm ways to stay active and connected that feel comfortable.”
Genetics (APOE)
Client: “Alzheimer’s runs in my family. Should I get tested?”
Coach: “It’s a big question. I can’t interpret genetic tests, but I can help you think through what you’d do with the information, and I can refer you to a genetic counselor if you want testing. Either way, the same everyday habits still matter a lot.”
| Coaching in practice | |
|---|---|
| The 14 factors at a glance | |
| When discussing modifiable risk factors with clients, this simplified breakdown may help: | |
| Cardiovascular factors (protect your blood vessels): | |
| Hypertension, high cholesterol, diabetes, smoking, obesity | |
| Lifestyle factors (what you do every day): | |
| Physical inactivity, excessive alcohol, unhealthy diet, cognitive disengagement | |
| Social-emotional factors (connection and mental health): | |
| Social isolation, depression | |
| Sensory factors (stay connected to the world): | |
| Hearing loss, vision loss | |
| Environmental factors (some harder to control): | |
| Air pollution, traumatic brain injury, lower educational attainment |
[CHONK: Coaching Cognitive Health]
Supporting clients with brain health concerns¶
Brain health conversations often call for extra sensitivity, because they can bring up fear, grief, and a lot of “What if?” all at once. And if you feel yourself choosing your words a little more carefully here, that’s normal. (This stuff matters.)
Many clients carry deep fears about cognitive decline. Maybe they watched a parent live with dementia, they’ve noticed their own memory lapses, or they’re simply worried about what the future holds. Those fears are real, and they deserve to be named out loud.
Your role is to offer accurate information, practical support, and clear boundaries. You probably won't erase their fear, but you can help them feel less alone and more grounded in what's actually in their control.
Scope-safe language for cognitive health¶
Here’s the key scope reminder for health and wellness coaches (Chapter 1.5). You are NOT:
- Diagnosing cognitive impairment or dementia, interpreting cognitive test results, or providing dementia treatment
- Assuring clients they won't get dementia
You ARE:
- Providing evidence-based education about brain health and supporting lifestyle behaviors associated with cognitive health
- Helping clients navigate fear and uncertainty
- Recognizing when referral is needed
Language to use:
- "Research suggests that..." and "associated with lower risk" (not "this will prevent..." or "prevents")
- "We can focus on what's within your control" and "these healthy behaviors benefit you regardless of future cognitive outcomes"
- "If you're concerned about your memory, we can talk about when to see your doctor"
Language to avoid:
- "This will protect you from Alzheimer's" or "if you follow this program, you won't get dementia"
- "Your memory problems are probably just normal aging" (you can't determine this)
- "You don't need to see a doctor about that" (you can't rule out concerning causes)
Supporting clients with family history¶
Clients with a parent or sibling with dementia often carry significant anxiety. That makes sense, because they've seen what this can look like up close. Here are a few scope-safe ways to support them.
Acknowledge the fear (dialogue-style):
Client: "My mom had dementia, and I can’t stop thinking it could happen to me."
Coach: "It makes complete sense that you'd be thinking about this. Watching your mother's decline was incredibly difficult, and worrying about your own future is natural."
Provide context:
Client: "Does having a parent with Alzheimer's mean I'm going to get it too?"
Coach: "Having a parent with Alzheimer's does increase risk, but it's not destiny. Most dementia is not purely genetic, and lifestyle factors play a significant role. Some research suggests lifestyle interventions may be particularly important for those with family history."
Focus on action:
Client: "So what can I actually do?"
Coach: "Rather than focusing on what you can't control, we can work together on what you can. Exercise, sleep, social connection, and managing cardiovascular health all matter for your overall wellbeing, and they may support brain health too."
Avoid false reassurance:
Don’t say "You'll be fine" or "You won't get dementia." You can’t promise that. Instead, you might say: "We're going to do everything we can to support your health and give you the best possible foundation." (Honest and supportive is the goal.)
Handling dementia fear conversations¶
These can be some of the most emotionally charged conversations you’ll have as a coach. If a client is scared, they may not be ready for information right away, and that’s okay. Often, they need to feel heard before anything else lands. (You don’t have to rush this.)
-
Listen fully before responding. Often people need to express fear before they can hear information, so don’t rush to reassure.
-
Validate the emotion: "These concerns are really common, and they make sense." (Because they do.)
-
Explore what's driving the fear: Is it a specific memory lapse, family history, or a recent diagnosis of a friend? Their answer guides what you do next.
-
Distinguish normal aging from concerning signs:
- Normal: Occasionally forgetting a word, misplacing keys, needing more time to learn new things
-
Concerning: Getting lost in familiar places, difficulty having conversations, personality changes, trouble with familiar tasks
-
Provide accurate information about what’s known and unknown.
-
Return focus to what they can do: "Regardless of what the future holds, these healthy behaviors are good for you now and may support your brain health over time."
-
Know when to refer (see below).
When to refer: recognizing warning signs¶
It’s appropriate to encourage medical evaluation when a client reports symptoms that could be more than everyday forgetfulness. If you’re unsure, leaning toward referral is usually the right call. (That’s you staying in scope and putting safety first.)
As a coach, encourage medical evaluation when clients report:
Memory concerns that:
- Interfere with daily activities, are noticed by others (not just the client), or represent a change from previous function
- Include forgetting recently learned information, important dates, or events
- Lead to repeatedly asking the same questions
Other cognitive changes:
- Difficulty planning, organizing, or solving problems
- Trouble completing familiar tasks, or confusion about time or place
- Visual-spatial issues (beyond normal vision changes)
- Language problems (speaking or writing)
- Misplacing things and being unable to retrace steps
- Poor judgment, withdrawal from work or social activities, or changes in mood or personality
The referral conversation:
Avoid downplaying it ("It’s probably nothing"), trying to rule things out yourself, or accidentally talking someone out of getting checked.
A scope-safe example (dialogue):
Coach: "You mentioned you’ve been getting lost on familiar routes, and your husband has noticed some changes. That sounds scary."
Client: "Yeah. I keep hoping it’s just stress, but… I don’t know."
Coach: "It could be stress, and it could be a lot of other things too. The important part is that many causes are treatable, but you usually need a medical evaluation to figure out what’s going on. I think it would be worth talking with your doctor. Would you be willing to make an appointment?"
Client: "I guess so. I’m nervous."
Coach: "Totally understandable. If you want, we can talk through what you might say, what questions to ask, and how to make the appointment feel more manageable." (Support without diagnosing.)
Important: Studies show that only about 26 percent of older adults who screen positive for cognitive issues accept referral for evaluation. Knowledge about cognitive impairment predicts acceptance. Your role in educating clients about the importance of evaluation, and the treatability of many causes, can help. If a client resists or feels embarrassed, you’re not saying it wrong. This is hard, and that’s okay.
Integrating brain health into Deep Health coaching¶
Brain health isn’t separate from overall health. It’s woven into every Deep Health dimension, which means you rarely have to “add” brain health as an extra project. In many cases, you’re already doing it. (Good news: you don’t have to make this more complicated than it is.)
Physical: Exercise, sleep, nutrition, and cardiovascular health all affect brain function
Mental/Cognitive: Cognitive stimulation, learning, and challenge
Emotional: Mood regulation, stress management, and depression prevention
Social: Connection, relationships, and community involvement
Existential: Purpose, meaning, and engagement with life
Environmental: Air quality, noise, and safety from head injury
When coaching for brain health, you’re really coaching for Deep Health, with particular attention to the cognitive dimension. Everything interconnects.
Brain health without inducing anxiety¶
Some clients get anxious when discussing brain health, and they start worrying about every forgotten name or missed appointment. If that’s your client, reassure them that occasional lapses happen to everyone, and then help them zoom out to patterns and actions. (This is a lot to take in, and that’s okay.)
-
Normalizing some forgetfulness: "Everyone forgets things sometimes. Occasional lapses are normal, especially when you're stressed or distracted."
-
Focusing on overall patterns: "Rather than worrying about individual incidents, we look at overall patterns over time."
-
Emphasizing the positive: "The fact that you're focused on brain health and taking action is itself protective. Stress and worry are more harmful than occasional forgetfulness."
-
Setting realistic expectations: "The goal isn't perfect memory, it's building a healthy foundation that supports your brain over time."
-
Redirecting rumination: "When you notice yourself worrying about your memory, try redirecting to one positive action you can take today."
Coaching in practice: Sample scripts for brain health conversations¶
The scenario: Clients bring high-stakes questions about brain health, supplements, and everyday forgetfulness.
Avoid offering guarantees, or jumping straight to supplements without acknowledging the limits of our knowledge and the importance of the fundamentals.
✅ Use honest, scope-safe language and redirect to foundational habits, while staying curious about what the client is really worried about.
Client: "What should I be doing to prevent Alzheimer's?"
Coach: "That’s an important question, and I’m glad you asked. I also want to be honest: we can’t guarantee prevention of any disease, including Alzheimer’s. What we can do is focus on the lifestyle factors that research shows influence brain health. The good news is that the same habits that support your brain also support your whole body, like exercise, quality sleep, healthy eating, social connection, stress management, and taking care of cardiovascular health. Which of these feels most manageable to start with?"
Client: "Should I be taking supplements for my brain?"
Coach: "Some supplements show modest benefits, and omega-3s have the most evidence. I’d still put supplements in the 'nice-to-have, not need-to-have' category, because the biggest wins come from the foundational habits like exercise, sleep, diet, and connection. Think of those as the main course, and supplements as seasoning. I’d want the main course to be solid first."
Client: "I forgot my neighbor's name and I'm worried something's wrong with me."
Coach: "That’s frustrating. Occasional word-finding difficulty is pretty common, especially when we’re tired or stressed. What concerns me more is when someone gets lost in familiar places, can’t follow conversations, or when other people notice consistent changes. Zooming out a bit, how has your overall cognitive function been? Any other changes you’ve noticed?"
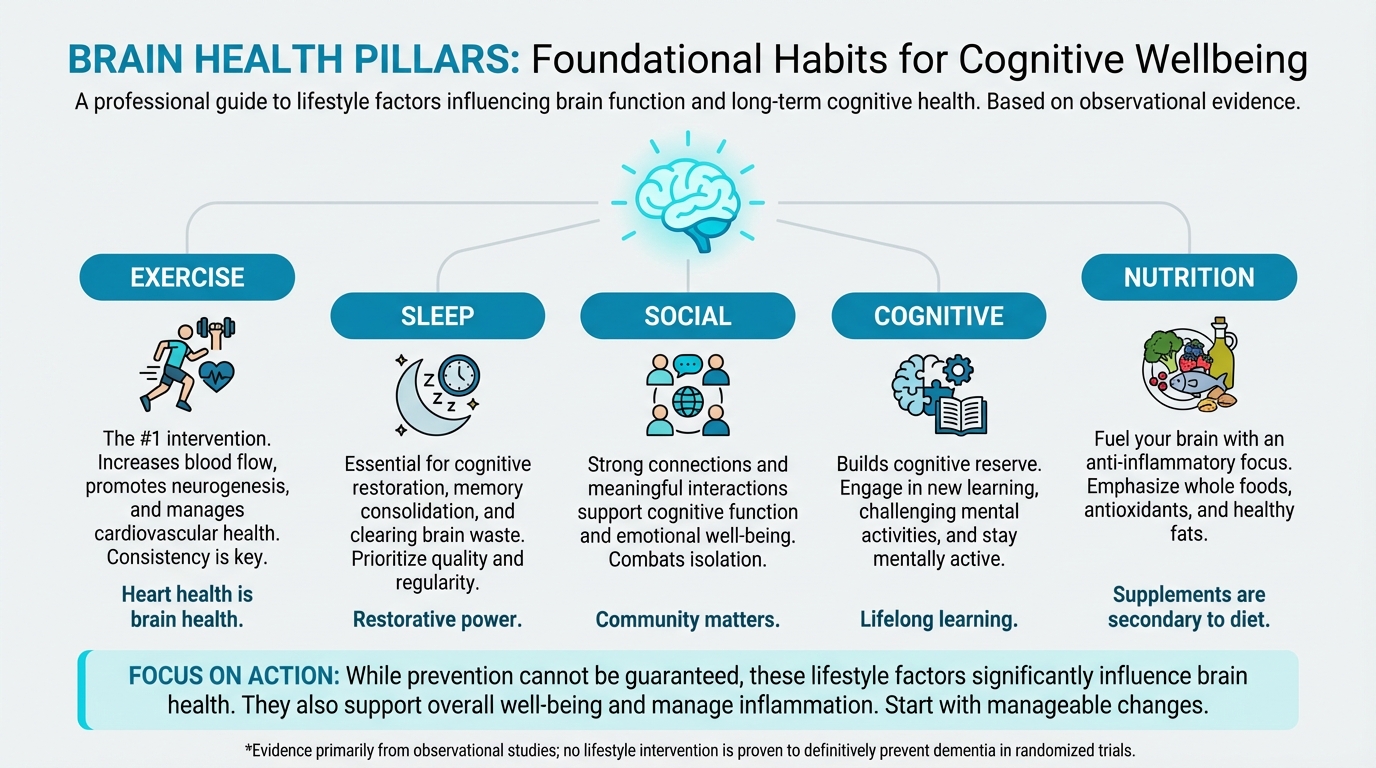
Figure: Exercise, sleep, social, cognitive, nutrition
[CHONK: Study guide questions]
Study guide questions¶
Use these questions to think through the material and get ready for the chapter exam. They're optional, but we recommend answering at least a few as part of your active learning process.
- What is cognitive reserve, and how is it built across the lifespan?
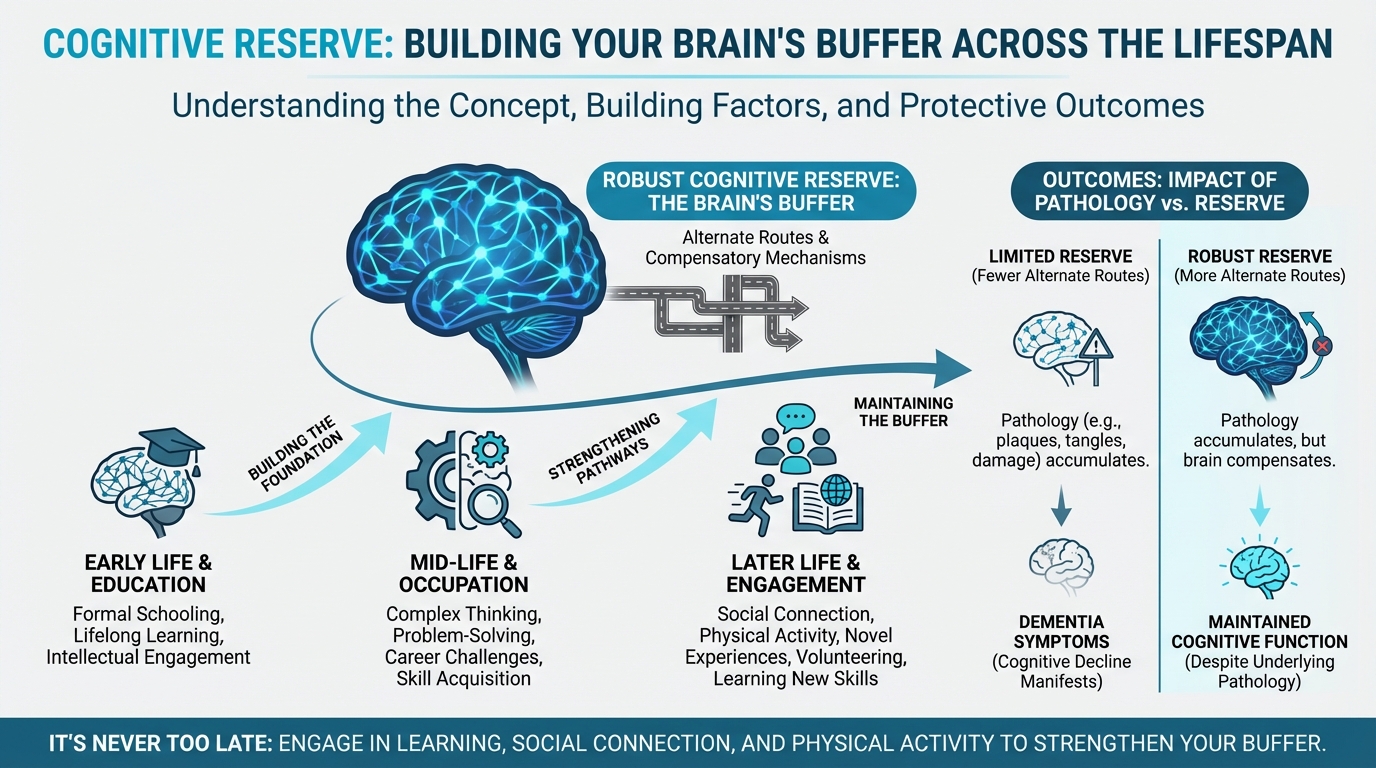
Figure: Building reserve across lifespan
-
According to the 2024 Lancet Commission, what percentage of dementia cases might be prevented or delayed by addressing modifiable risk factors? What caveats should you keep in mind about this number?
-
Why is exercise considered the #1 brain health intervention? What dose and type appear most beneficial?
-
Sketch a short (3–5 line) coach–client conversation that explains why sleep matters for brain health in accessible language.
-
What's the difference between what coaches can and cannot promise regarding brain health interventions?
-
List at least five of the 14 modifiable risk factors identified by the Lancet Commission. Which are cardiovascular-related?
-
Create a brief coach–client exchange that covers when you’d refer someone for medical evaluation of cognitive concerns. What warning signs would prompt referral?
-
Write a few lines of dialogue showing how you’d support a client with a significant family history of dementia who feels anxious about their own cognitive future.
Self-reflection questions:
-
Which of the 14 modifiable risk factors for dementia apply to you personally? Which one would you prioritize addressing first?
-
When did you last learn something genuinely new and challenging? Building cognitive reserve requires pushing beyond your comfort zone, not just doing crossword puzzles.
Works cited¶
Want to dig into the research? Here are the sources cited in this chapter. (You don’t need to read all of them to do well on the exam.)
References¶
-
Livingston G, Huntley J, Liu KY, Costafreda SG, Selbæk G, Alladi S, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. The Lancet. 2024;404(10452):572-628. doi:10.1016/s0140-6736(24)01296-0
-
Desai R, John A, Saunders R, Marchant NL, Buckman JEJ, Charlesworth G, et al. Examining the Lancet Commission risk factors for dementia using Mendelian randomisation. BMJ Mental Health. 2023;26(1):e300555. doi:10.1136/bmjment-2022-300555
-
Singh B, Bennett H, Miatke A, Dumuid D, Curtis R, Ferguson T, et al. Effectiveness of exercise for improving cognition, memory and executive function: a systematic umbrella review and meta-meta-analysis. British Journal of Sports Medicine. 2025;59(12):866-876. doi:10.1136/bjsports-2024-108589
-
Zhang M, Fang W, Wang J. Effects of human concurrent aerobic and resistance training on cognitive health: A systematic review with meta-analysis. International Journal of Clinical and Health Psychology. 2025;25(1):100559. doi:10.1016/j.ijchp.2025.100559
-
Liu H, Sun Z, Zeng H, Han J, Hu M, Mao D, et al. Meta-analysis of the effects of multi-component exercise on cognitive function in older adults with cognitive impairment. Frontiers in Aging Neuroscience. 2025;17. doi:10.3389/fnagi.2025.1551877
-
Wang Y, Li F, Cao S, Jia J. Dose- and pattern- physical activity is associated with lower risk of dementia. The Journal of Prevention of Alzheimer's Disease. 2025;12(7):100223. doi:10.1016/j.tjpad.2025.100223
-
Hu M, Zhang K, Su K, Qin T, Shen H, Deng H. Unveiling the link between physical activity levels and dementia risk: Insights from the UK Biobank study. Psychiatry Research. 2024;336:115875. doi:10.1016/j.psychres.2024.115875
-
Barnes LL, Dhana K, Liu X, Carey VJ, Ventrelle J, Johnson K, et al. Trial of the MIND Diet for Prevention of Cognitive Decline in Older Persons. New England Journal of Medicine. 2023;389(7):602-611. doi:10.1056/nejmoa2302368
-
Chen H, Dhana K, Huang Y, Huang L, Tao Y, Liu X, et al. Association of the Mediterranean Dietary Approaches to Stop Hypertension Intervention for Neurodegenerative Delay (MIND) Diet With the Risk of Dementia. JAMA Psychiatry. 2023;80(6):630. doi:10.1001/jamapsychiatry.2023.0800
-
Barros MI, Brandão T, Irving SC, Alves P, Gomes F, Correia M. Omega-3 Polyunsaturated Fatty Acids and Cognitive Decline in Adults with Non-Dementia or Mild Cognitive Impairment: An Overview of Systematic Reviews. Nutrients. 2025;17(18):3002. doi:10.3390/nu17183002
-
Suh SW, Lim E, Burm S, Lee H, Bae JB, Han JW, et al. The influence of n-3 polyunsaturated fatty acids on cognitive function in individuals without dementia: a systematic review and dose–response meta-analysis. BMC Medicine. 2024;22(1). doi:10.1186/s12916-024-03296-0
-
Luchetti M, Aschwanden D, Sesker AA, Zhu X, O’Súilleabháin PS, Stephan Y, et al. A meta-analysis of loneliness and risk of dementia using longitudinal data from >600,000 individuals. Nature Mental Health. 2024;2(11):1350-1361. doi:10.1038/s44220-024-00328-9
-
Huang AR, Roth DL, Cidav T, Chung S, Amjad H, Thorpe RJ, et al. Social isolation and 9‐year dementia risk in
<scp>community‐dwelling</scp>
Medicare beneficiaries in the United States. Journal of the American Geriatrics Society. 2023;71(3):765-773. doi:10.1111/jgs.18140 -
Sutin AR, Luchetti M, Stephan Y, Terracciano A. Purpose in life and cognitive health: a 28-year prospective study. International Psychogeriatrics. 2024;36(10):956-964. doi:10.1017/s1041610224000383
-
Buchman AS. Effect of Purpose in Life on the Relation Between Alzheimer Disease Pathologic Changes on Cognitive Function in Advanced Age. Archives of General Psychiatry. 2012;69(5):499. doi:10.1001/archgenpsychiatry.2011.1487
-
Zhou B, Wang Z, Zhu L, Huang G, Li B, Chen C, et al. Effects of different physical activities on brain-derived neurotrophic factor: A systematic review and bayesian network meta-analysis. Frontiers in Aging Neuroscience. 2022;14. doi:10.3389/fnagi.2022.981002
-
Resende-Silva S, de Resende-Neto AG, Vasconcelos ABS, Pereira-Monteiro MR, Pantoja-Cardoso A, Santana Santos LE, et al. Functional training improves cognitive function, functional fitness, and BDNF levels in older women with mild cognitive impairment: a randomized controlled trial. Frontiers in Physiology. 2025;16. doi:10.3389/fphys.2025.1638590
-
Xu C, Bi S, Zhang W, Luo L. The effects of creatine supplementation on cognitive function in adults: a systematic review and meta-analysis. Frontiers in Nutrition. 2024;11. doi:10.3389/fnut.2024.1424972
-
Sandkühler JF, Kersting X, Faust A, Königs EK, Altman G, Ettinger U, et al. The effects of creatine supplementation on cognitive performance - a randomised controlled study. 2023. doi:10.1101/2023.04.05.23288194
-
EFSA NDA Panel. Evaluation of health claims related to creatine and cognitive function. EFSA Journal; 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11574456/
-
Syed M, Lum JAG, Byrne LK, Skvarc D. Examining Working Memory Training for Healthy Adults—A Second-Order Meta-Analysis. Journal of Intelligence. 2024;12(11):114. doi:10.3390/jintelligence12110114
-
Hampshire A, Sandrone S, Hellyer PJ. A Large-Scale, Cross-Sectional Investigation Into the Efficacy of Brain Training. Frontiers in Human Neuroscience. 2019;13. doi:10.3389/fnhum.2019.00221
-
Schwartz HE, Bay CP, McFeeley BM, Krivanek TJ, Daffner KR, Gale SA. The Brain Health Champion study: Health coaching changes behaviors in patients with cognitive impairment. Alzheimer's & Dementia: Translational Research & Clinical Interventions. 2019;5(1):771-779. doi:10.1016/j.trci.2019.09.008
-
Laukkanen T, Kunutsor S, Kauhanen J, Laukkanen JA. Sauna bathing is inversely associated with dementia and Alzheimer's disease in middle-aged Finnish men. Age and Ageing. 2016;46(2):245-249. doi:10.1093/ageing/afw212
-
Knekt P, Järvinen R, Rissanen H, Heliövaara M, Aromaa A. Does sauna bathing protect against dementia?. Preventive Medicine Reports. 2020;20:101221. doi:10.1016/j.pmedr.2020.101221
-
Wei BZ, et al. The Relationship of Omega-3 Fatty Acids with Dementia and Cognitive Decline: Evidence from Prospective Cohort Studies and Meta-Analyses. Am J Clin Nutr; 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10447496/
-
Harrington KD, Vasan S, Kang Je, Sliwinski MJ, Lim MH. Loneliness and Cognitive Function in Older Adults Without Dementia: A Systematic Review and Meta-Analysis. Journal of Alzheimer's Disease. 2023;91(4):1243-1259. doi:10.3233/jad-220832
-
Salinas J, Beiser A, Himali JJ, Satizabal CL, Aparicio HJ, Weinstein G, et al. Associations between social relationship measures, serum brain‐derived neurotrophic factor, and risk of stroke and dementia. Alzheimer's & Dementia: Translational Research & Clinical Interventions. 2017;3(2):229-237. doi:10.1016/j.trci.2017.03.001
-
Iso-Markku P, Aaltonen S, Kujala UM, Halme H, Phipps D, Knittle K, et al. Physical Activity and Cognitive Decline Among Older Adults. JAMA Network Open. 2024;7(2):e2354285. doi:10.1001/jamanetworkopen.2023.54285
-
Baker LD, Espeland MA, Whitmer RA, Snyder HM, Leng X, Lovato L, et al. Structured vs Self-Guided Multidomain Lifestyle Interventions for Global Cognitive Function. JAMA. 2025;334(8):681. doi:10.1001/jama.2025.12923
-
Deng C, Shen N, Li G, Zhang K, Yang S. Digital Isolation and Dementia Risk in Older Adults: Longitudinal Cohort Study. Journal of Medical Internet Research. 2025;27:e65379. doi:10.2196/65379