Unit 3: Advanced Topics & Disease Prevention¶
Chapter 3.20: Supporting Women's Hormonal Health¶
[CHONK: 1-minute summary]
[CHONK: Introduction and Context]
Why this chapter matters¶
At some point, every woman goes through menopause.
Menopause isn't a disease or a disorder; it's a normal biological transition, and yet it affects nearly every system in the body: sleep, mood, bone health, cardiovascular risk, body composition, and energy levels. For some women, the changes are subtle. For others, they're profound.
As a coach, you'll work with women navigating this transition. Some will breeze through with minimal symptoms. Others will experience changes that significantly affect their daily lives, their training, their relationships, and their sense of self.
(If you're a woman yourself, you may be navigating some of this personally. It can actually make you a better coach.)
This chapter gives you the knowledge to support these clients effectively, and the wisdom to know where your support ends and medical care begins.
The key distinction for this chapter is that hormone replacement therapy (HRT) is a medical decision that sits firmly outside your scope. You cannot recommend for or against HRT, interpret hormone labs, or advise on formulations or dosages.
Here’s how that can sound in practice.
What not to do
Client: “Should I start HRT?”
Coach: “Yes, you should; your labs look low.”
Better
Client: “Should I start HRT?”
Coach: “That’s an important conversation to have with your clinician. I can’t recommend for or against HRT, but I can help you make sense of what you’re experiencing, work on the lifestyle factors that matter, and help you prepare questions for your healthcare provider.”
But here's what you can do: understand what's happening physiologically, help clients with lifestyle factors that genuinely matter, and know when to encourage conversations with healthcare providers.
That’s what this chapter teaches you to do, and it matters a lot.
Learning objectives¶
By the end of this chapter, you'll be able to:
- Explain the physiology of perimenopause and menopause, including key hormonal changes and their effects on multiple body systems
- Discuss HRT with appropriate scope: educating about evidence without recommending for or against
- Describe training and nutrition adjustments that support women through hormonal transitions
- Support clients through menopause without overstepping into medical practice
- Identify when hormonal symptoms require referral to appropriate medical specialists
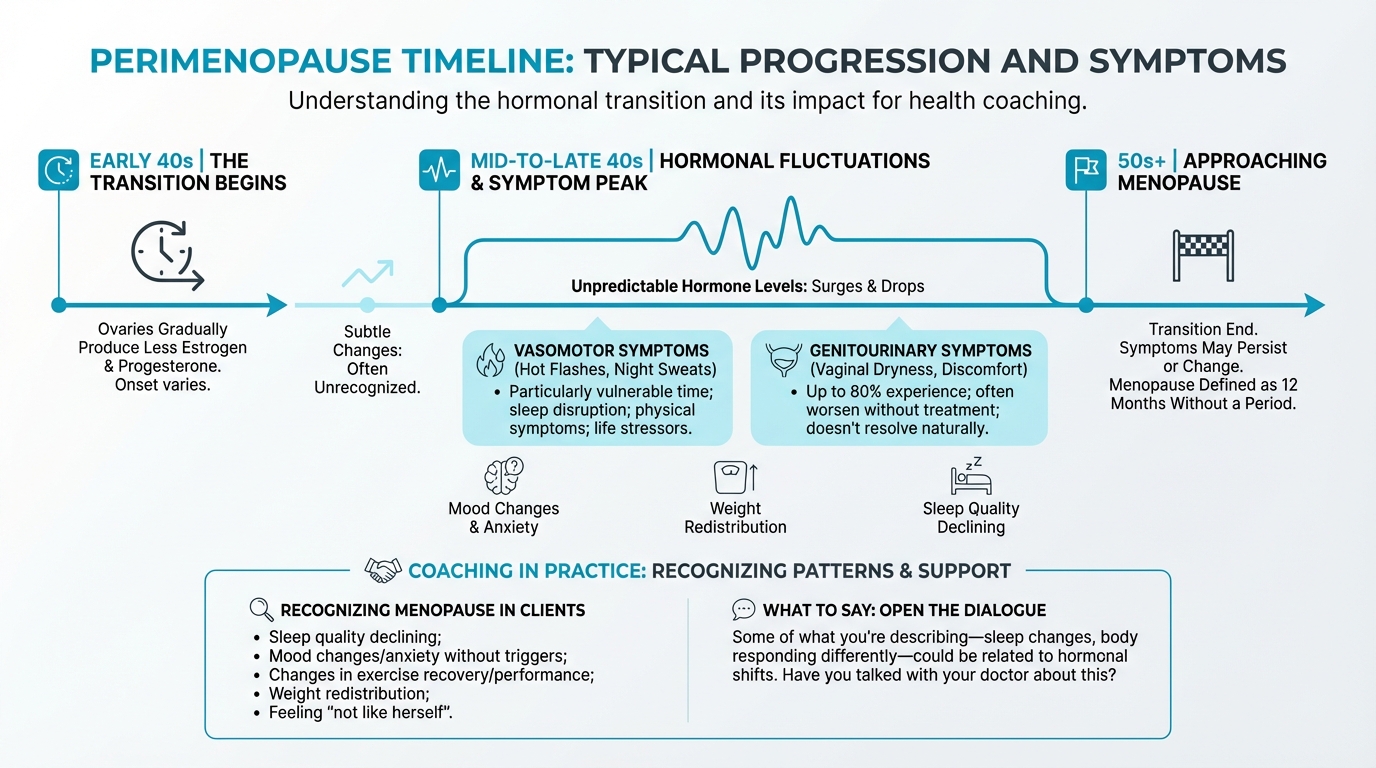
Figure: Typical progression and symptoms
[CHONK: The Menopause Transition]
What happens during menopause¶
It helps to start with clear definitions, because these terms get used loosely, and being precise here makes everything else easier to understand.
Perimenopause: The transition begins¶
Perimenopause, also called the menopausal transition, is the time leading up to menopause. It typically begins in a woman's mid-to-late 40s, though it can start earlier.
During perimenopause, the ovaries gradually produce less estrogen and progesterone, but the shift usually isn’t smooth or linear. Hormone levels can fluctuate unpredictably, sometimes surging higher than ever before and then dropping, and those ups and downs drive many of the symptoms women experience.
How long does it last?
- For most women, the median duration is about four years, though a range of two to eight years is common.
- Some women experience a longer transition (about 10 to 14 years), and starting earlier tends to predict a longer transition.
The STRAW+10 staging system (Stages of Reproductive Aging Workshop) defines perimenopause as spanning from the onset of menstrual cycle changes through 12 months after the final menstrual period.
Menopause: A specific moment¶
Menopause itself is a single point in time: the moment when a woman has gone 12 consecutive months without a menstrual period (assuming no other cause).
- Average age is 51-52 years, with a typical range of 45-58 years
- Menopause is defined retrospectively, meaning you only know it happened after a year without periods
Types of menopause¶
Not all menopause is the same:
Natural menopause occurs when estrogen and progesterone decline naturally with aging.
Surgical menopause happens when the ovaries are removed (oophorectomy). Because hormone levels drop suddenly rather than gradually, symptoms often begin immediately and may be more intense.
Premature menopause (or premature ovarian insufficiency) occurs before age 40. This affects about 1 in 100 women before 40 and 1 in 1,000 before 30. Risk factors include certain medical conditions, treatments like chemotherapy, smoking, and genetic factors.
The hormones involved¶
Several hormones change during this transition, and each one tells you something slightly different about what the body is doing. You don’t need to memorize all of these names. You just want the big picture.
Estrogen is actually a family of hormones: estrone (E1), estradiol (E2), and estriol (E3). Estradiol is the primary estrogen during reproductive years. After menopause, estrone becomes dominant but at much lower overall levels.
Progesterone drops as ovulation becomes irregular and then ceases entirely after menopause.
Follicle-stimulating hormone (FSH) rises as the brain tries to signal the ovaries to produce more estrogen, which is why high FSH levels can help confirm menopausal status.
Luteinizing hormone (LH) also increases during the transition.
Why these changes affect the whole body¶
Estrogen receptors exist throughout the body, not just in reproductive organs, so when estrogen levels drop, multiple systems feel the effects. From a coaching perspective, that’s helpful, because there are lots of entry points for support.
- Brain: Helps regulate mood, cognitive function, and temperature control
- Cardiovascular system: Supports blood vessel function and cholesterol metabolism
- Bones: Plays a central role in bone remodeling and density maintenance
- Skin: Influences collagen production and moisture retention
- Urogenital tract: Affects vaginal tissue health and urinary function
- Muscles: Contributes to protein synthesis and muscle maintenance
This is why menopause symptoms extend far beyond hot flashes.
| For DIY Learners |
|---|
| Applying this to yourself: If you're a woman in your 40s or beyond, you may be navigating this transition right now, or preparing for it. Understanding what's happening physiologically can be genuinely empowering. Those confusing symptoms (the sleep disruption, the brain fog, the body changes that don't respond to your usual strategies) start to make sense when you understand the systemic nature of hormonal shifts. And if you're not yet in perimenopause, knowing what to expect can help you prepare and recognize early signs. This isn't about anxiety; it's about being informed. |
Common symptoms and their impact¶
Vasomotor symptoms: Hot flashes and night sweats¶
These are the symptoms most associated with menopause:
- About 57 percent of women aged 40-64 experience vasomotor symptoms, and 15-20 percent experience moderate-to-severe symptoms
- Symptoms can persist for seven or more years after menopause, and prevalence and severity vary significantly by individual and demographic factors
Hot flashes involve a sudden sensation of heat, often accompanied by flushing and sweating. When they occur at night (night sweats), they can significantly disrupt sleep.
Sleep disruption¶
Sleep problems are extremely common:
- 40-60 percent of menopausal women report significant sleep problems, and about half of postmenopausal women meet criteria for at least one sleep disorder
- About 26 percent experience symptoms consistent with clinical insomnia, and restless legs syndrome also shows high prevalence
Sleep disruption often connects to night sweats but can occur independently. Some women wake from hot flashes, while others simply have difficulty falling asleep or staying asleep even without obvious triggers.
Why sleep disruption matters so much:
Poor sleep tends to compound every other symptom, affecting:
- Mood regulation, emotional resilience, and cognitive function (worsening "brain fog")
- Appetite hormones (increasing hunger, particularly for high-calorie foods) and recovery from exercise
- Energy, motivation for healthy behaviors, and immune function
This is why sleep environment and sleep hygiene should be early priorities when coaching menopausal clients. When sleep improves, it often creates a positive cascade into other areas.
Mood changes¶
Depression and anxiety occur more frequently during the menopausal transition:
- The perimenopause appears to be a particularly vulnerable time
- Changes relate partly to hormonal fluctuations and partly to life circumstances
- Sleep disruption, physical symptoms, and life stressors all contribute
Cognitive changes¶
Many women report cognitive changes, often called "brain fog":
- 44-62 percent of perimenopausal women report memory problems, and 60-70 percent of midlife women report memory or concentration concerns
- Objective testing shows small but reliable declines in verbal memory and executive function during the transition, though for most women, performance remains within normal limits
Current guidelines do not recommend hormone therapy specifically for cognitive symptoms.
Body composition changes¶
Menopause is associated with shifts in body composition:
- Average weight gain of 2-3 kg during the transition, along with a shift toward central and visceral fat accumulation
- Decline in lean muscle mass; these changes occur partly from hormonal shifts and partly from aging itself
Bone loss¶
The skeletal impact is significant:
- Estrogen helps maintain bone density, and its decline accelerates bone loss
- Women can lose 1-5 percent of bone mineral density per year in the first 5-7 years after menopause
- About one in two women over 50 will experience an osteoporotic fracture, and hip fractures carry 12-20 percent one-year mortality in older women
Those last two stats can feel scary to read. The point here isn’t to panic, but to recognize why bone-supporting habits (and appropriate medical screening) matter so much in this life stage.
Genitourinary changes¶
Changes to vaginal and urinary tissue are common but often underdiscussed:
- Up to 80 percent of menopausal women experience genitourinary symptoms, including vaginal dryness, discomfort during sex, and urinary symptoms
- Unlike hot flashes, these symptoms typically don't resolve over time. They often worsen without treatment
Many clients feel embarrassed or unsure how to bring up dryness, discomfort during sex, or urinary symptoms, which is exactly why calm, matter-of-fact language from a coach can be so helpful.
Cardiovascular changes¶
Menopause accelerates cardiovascular risk:
- Loss of estrogen's protective effects on blood vessels
- Shifts in cholesterol patterns (increased LDL, decreased HDL)
- Increased visceral fat and insulin resistance
- The "cardiovascular gap" between men and women narrows after menopause
Individual variation is enormous¶
Perhaps the most important thing to understand is this: no two women experience menopause the same way.
Some women have minimal symptoms, while others are significantly affected, and duration, severity, and which symptoms predominate can vary widely. Race, ethnicity, body composition, lifestyle factors, and genetics all influence the experience.
Research shows meaningful differences across populations:
- African-American women tend to have longer menopausal transitions and more severe vasomotor symptoms
- Smoking is associated with earlier menopause onset
- Higher body mass index is associated with later onset
- Geographic and cultural factors influence both symptom reporting and treatment-seeking
This variation means cookie-cutter approaches don't work. What helps one client may not help another, so your role is to understand the individual in front of you (her specific symptoms, her context, her goals) and adapt your support accordingly.
Coaching in practice: Recognizing menopause in your clients¶
The scenario: Your client is in her early-to-mid 40s, and she’s noticing changes in sleep, mood, and how her body responds to training, but she hasn’t connected any of this to hormones.
She might say things like, "I'm not sleeping as well," "I feel more anxious for no reason," or "My workouts wipe me out now," without realizing these shifts could be part of the menopausal transition.
Common patterns to notice include:
- Sleep quality declining even though her schedule, stress, and habits haven’t changed much
- Mood shifting toward more irritability or anxiety, without a clear trigger she can point to
- Recovery feeling slower than usual, or workouts that used to feel manageable suddenly feeling much harder
- Weight redistributing toward the midsection despite consistent eating and training habits
- A general sense of feeling “off,” or "not like herself," that’s hard for her to explain
What NOT to do:
❌ Tell her, "Oh, this is definitely perimenopause," or suggest specific medical treatments.
Why it doesn't work: You're stepping into diagnosing and medical decision-making, which is outside your scope.
What TO do:
✅ Get curious about patterns, reflect what you're hearing, and gently suggest a medical conversation, without labeling or diagnosing.
Sample dialogue:
Client: "I'm doing everything the same, but I'm not sleeping, I'm more on edge, and my workouts feel so much harder. I just don't feel like myself."
Coach: "I hear how much this is affecting you, and that 'not like myself' feeling can be really unsettling. You're noticing changes in sleep, mood, and recovery, and those can have lots of possible causes."
Client: "Yeah, I keep wondering if I'm just stressed or if something else is going on."
Coach: "It could be stress, and it could also be related to hormonal shifts that are common for women in their 40s and 50s. I can't tell you exactly what's happening because that’s beyond my role, but it does sound worth talking through with your doctor."
Client: "I hadn't even thought about hormones. What should I say to my doctor?"
Coach: "You might share exactly what you told me: the changes in your sleep, mood, recovery, and how long they've been going on. If you'd like, we can jot down a few notes or questions for your appointment. And whatever your doctor finds, we can keep working on your sleep, training, and nutrition together."
Why these conversations are emotionally loaded¶
Menopause touches on some of our culture's deepest anxieties: aging, femininity, identity, and loss.
When a client realizes that hormonal changes might be behind her symptoms, she's not just getting information. She's potentially confronting a shift in how she sees herself. For some women, this realization brings relief ("Oh, there's a reason for all this"). For others, it brings grief or fear.
As a coach, you don't need to fix these feelings, but you can make space for them and keep the conversation grounded. Sometimes the most powerful thing you can do is acknowledge: "It's normal if this brings up complicated feelings, because you're not just dealing with symptoms; you're navigating a transition that affects how you feel in your body."
[CHONK: HRT - What Coaches Should Know]
Hormone replacement therapy: An educational overview¶
Clients are going to have questions about HRT, because they’ll see headlines, hear friends’ experiences, and wonder what (if anything) they should do next. Your job is to understand HRT well enough to have a calm, informed conversation and to keep one thing front and center: HRT decisions belong to medical professionals. (That boundary protects you and your client.)
A medical decision, not a coaching decision¶
First, a quick scope check, because this topic can get blurry fast.
Coaches CAN:
- Explain what HRT is in general terms
- Share that research exists and continues to evolve
- Encourage clients to discuss HRT with their healthcare providers
- Support clients who are using HRT (without commenting on whether they should be)
- Support clients who choose not to use HRT
Coaches CANNOT:
- Recommend for or against HRT
- Suggest specific formulations, doses, or delivery methods
- Interpret hormone lab results
- Advise on starting, stopping, or adjusting HRT
- Express opinions about whether a client "should" be on HRT
Here’s a simple way to handle the most common question as a coach:
Client: “Should I take HRT?”
Coach: “That’s a medical decision between you and your healthcare provider. I can absolutely support you either way with lifestyle factors, but I’m not qualified to advise on hormone therapy.”
The WHI controversy and how understanding evolved¶
If you want context for why HRT conversations can feel emotionally charged, it helps to know about the Women’s Health Initiative (WHI).
In 2002, the WHI (a large randomized trial) was stopped early after researchers found increased risks of breast cancer, heart disease, and stroke in women taking combined estrogen-progestin therapy. The headlines were intense, many women stopped therapy abruptly, and prescribing dropped dramatically.
Over time, though, researchers reanalyzed the data more carefully, and a more complex picture emerged. (Spoiler: it wasn’t just “HRT is good” or “HRT is bad.”)
What the reanalysis showed:
- Age and timing matter enormously. Women who started HRT closer to menopause (within about 10 years of menopause or before age 60) showed different patterns than women who started later.
- Formulation matters. Estrogen-only therapy (for women who've had a hysterectomy) showed different risks than combined estrogen-progestin therapy.
- Route matters. Transdermal (patch or gel) estrogen appears to have lower clotting risks than oral estrogen.
- Progestogen type matters. Micronized progesterone may carry lower breast cancer risk than synthetic progestins, though head-to-head randomized trial data are limited.
The "timing hypothesis"¶
One key concept that came out of the WHI reanalysis is the timing hypothesis (sometimes called the “critical window”):
Starting HRT within about 10 years of menopause onset or before age 60 is associated with a more favorable benefit-risk profile than starting later.
Major guidelines now reflect this. The North American Menopause Society, the Endocrine Society, and international cardiology guidelines all acknowledge this timing effect.
However (and this matters), the timing hypothesis doesn’t make HRT “safe” or “recommended.” It just means the risk-benefit calculation can look different depending on when therapy starts, and individual factors still drive the decision.
This is complex, and biology doesn't always offer a clear, one-size-fits-all answer.
What HRT involves (educational overview)¶
HRT typically includes:
Estrogen: Replaces declining estrogen levels. Available as:
- Oral pills
- Transdermal patches
- Topical gels or creams
- Vaginal preparations (for local symptoms only)
Progestogen: Required for women who have a uterus to protect against endometrial cancer. Options include:
- Synthetic progestins
- Micronized (natural) progesterone
Testosterone: Sometimes prescribed for sexual desire concerns. We'll discuss this separately below.
The choice of formulation, route, and dose depends on individual factors. That’s a medical determination, not a coaching one. (And you don’t have to memorize product lists to be helpful.)
Current evidence: What research shows¶
Here’s what the current research suggests, with the usual caveats (different populations, different formulations, different timelines):
For symptom relief:
- HRT remains the most effective treatment for vasomotor symptoms
- It effectively treats genitourinary symptoms of menopause
- Effects on mood and sleep vary by individual
For bone health:
- HRT prevents early postmenopausal bone loss
- It reduces fracture risk during use
For cardiovascular outcomes:
- The picture is complex and depends heavily on timing
- Early initiation (near menopause) is associated with more favorable cardiovascular signals
- Late initiation increases cardiovascular risks
- HRT is not recommended for primary cardiovascular disease prevention
For breast cancer:
- Risk depends on formulation and duration
- Estrogen-only therapy shows little or no increase in breast cancer risk
- Combined therapy with synthetic progestins increases risk modestly
- Micronized progesterone may carry lower risk than synthetic progestins (observational data)
- Risk appears to decline after discontinuation
For stroke and blood clots:
- HRT increases stroke risk, particularly with oral formulations and older age
- Venous thromboembolism risk is elevated with oral therapy; transdermal routes appear safer
This section can feel pretty “risk-forward,” and that can be unsettling. That’s OK. A useful coaching stance is: “This is real, it’s individualized, and it deserves a medical conversation.” (Your steadiness helps.)
"Bioidentical" hormones: A note¶
You may hear clients ask about “bioidentical” hormones. The term is often used for hormones that are chemically identical to those the body produces.
Many FDA-approved HRT products are bioidentical, including transdermal estradiol patches and micronized progesterone.
The term is also sometimes used for custom-compounded preparations from compounding pharmacies. These preparations:
- Lack the regulatory oversight of FDA-approved products
- May have potency and quality variations
- Have not been shown to be safer or more effective than approved products
- Are not recommended by major guidelines over approved alternatives
The evidence is evolving¶
Honest conversations about HRT can be tricky because the evidence continues to evolve. Research on different formulations, routes, and timing is ongoing, and what we understand today may be refined by future studies.
If you’re feeling like the ground keeps shifting here, you’re not alone. Even clinicians have had to update their understanding over time.
This is exactly why HRT decisions belong with medical professionals who can integrate the latest evidence with an individual’s health history, symptoms, and risk factors.
Coaching in practice: "Should I take HRT?"¶
The scenario: Your client has been reading articles and talking with friends, and now she asks: "Should I take HRT?"
What NOT to do:
❌ Give a yes-or-no answer or share what you would do in her place.
❌ Say things like:
- "You should definitely consider HRT. It's much safer than people used to think."
- "I wouldn't take HRT if I were you."
- "Your hormones seem low, so you probably need HRT."
- "I think you'd really benefit from bioidentical hormones."
Why it doesn't work: You're stepping into medical decision-making and making assumptions about her health history and risks.
What TO do:
✅ Name your scope, validate the question, and redirect to a medical conversation, while staying available to support lifestyle changes.
Sample dialogue:
Client: "I've been reading so much about hormones, and honestly I'm confused. Should I take HRT?"
Coach: "That makes total sense. There’s a lot of information out there, and a lot of it sounds confident even when it disagrees. (You’re not doing anything wrong by feeling stuck.)"
Client: "Yeah, everyone seems to say something different."
Coach: "HRT is a medical decision that depends on your health history, your symptoms, and your risk factors, so it’s not something I can advise on directly. The best place to sort that out is with your doctor or a menopause specialist."
Client: "So you can't tell me if it's safe?"
Coach: "What I can tell you is that the research on HRT has evolved a lot over the years, and it’s worth having an informed conversation with your healthcare provider. If you’d like, I can help you think through questions to ask at that appointment, and whatever you and your doctor decide, I’m here to support you with the lifestyle pieces that matter either way." (And that part is very much in our lane.)
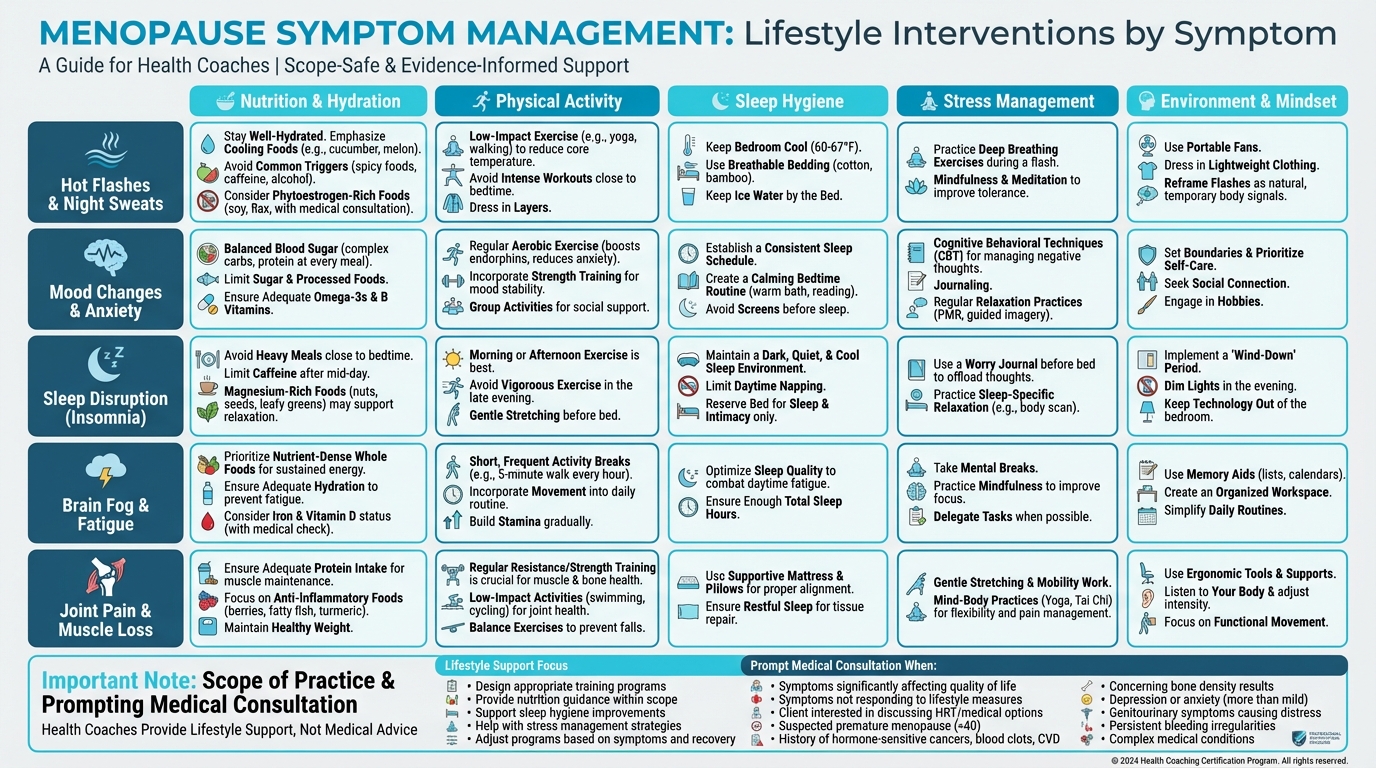
Figure: Lifestyle interventions by symptom
Testosterone for women: Brief note¶
You may hear clients ask about testosterone for women. The key points are:
- Testosterone is sometimes prescribed for hypoactive sexual desire disorder (HSDD) in postmenopausal women
- Clinical trials show modest improvements in sexual desire in selected women
- There is no good evidence that testosterone improves energy, mood, cognition, or general well-being in women
- Long-term safety data are limited
- It is not FDA-approved for use in women in the United States
Current guidelines recommend testosterone only for women with diagnosed HSDD after other causes have been excluded, with careful monitoring and time-limited treatment.
This is firmly a medical decision. As a coach, do not recommend testosterone to clients.
Emerging research: A mention¶
You may see headlines about interventions to delay menopause or "preserve ovarian function." Some examples:
mTOR inhibitors (like rapamycin): Early animal studies and a small pilot human trial suggest mTOR inhibitors might slow the activation of follicles in the ovaries. Larger human trials are planned but not complete.
Hyperbaric oxygen therapy (HBOT): Animal studies show some effects on ovarian markers, but no human clinical trials have demonstrated effects on menopause timing.
Big picture: No intervention has been proven in randomized human trials to delay natural menopause. These remain experimental areas of research. They are not ready for clinical application and are not something coaches should discuss as options.
[CHONK: Training Through the Transition]
Exercise for women during hormonal transitions¶
If there's one area where coaches can make a genuine difference for women in menopause, it's exercise. The evidence for exercise benefits during this transition is strong, and it's also solidly within coaching scope.
Why strength training matters more during menopause¶
As estrogen declines, women tend to face faster losses of both muscle mass and bone density, and strength training is one of the most direct ways to push back on both. (And no, this doesn’t mean everyone needs to become a powerlifter. We’re talking about appropriately challenging training.)
For muscle preservation:
- Sarcopenia (age-related muscle loss) accelerates after menopause, which is one reason strength work becomes more important over time
- Resistance training is the primary intervention we have to maintain and build muscle
- Postmenopausal women may need higher training volumes than premenopausal women to see similar muscle-building results
- In one study, postmenopausal women needed more than 6-8 sets per muscle group weekly to gain muscle mass, while premenopausal women gained mass at that volume
For bone health:
- Weight-bearing and resistance exercise stimulates bone remodeling
- High-impact activities (jumping, hopping) can provide an additional bone stimulus when they’re appropriate for the person doing them
- Meta-analyses show mixed-loading programs (combining impact exercise with resistance training) effectively preserve bone mineral density at the hip and spine
For metabolic health:
- Resistance training helps maintain metabolic rate by preserving muscle mass, improves insulin sensitivity, and, when it’s combined with aerobic exercise, positively affects body composition
| For DIY Learners |
|---|
| Applying this to yourself: If you're a woman approaching or in menopause, now is a great time to prioritize strength training if you haven’t already. This isn’t about aesthetics; it’s about bone health, metabolic resilience, and functional independence as you age. The research suggests you may need higher training volumes than you needed before to get the same results, and that isn’t failure. That’s biology. (You’re not “doing it wrong.”) Meet your body where it is, not where it was ten years ago. And if you’re not currently doing structured resistance training at least 2-3 times per week, consider this your friendly nudge to start. |
What the research shows¶
Here’s the big-picture takeaway from research on exercise during menopause.
Body composition:
- Resistance training tends to be most effective for maintaining or increasing lean mass
- Aerobic training tends to be most effective for reducing fat mass
- Combined programs usually deliver the best overall results
Bone mineral density:
- High-impact and high-intensity loading can help preserve bone
- Effects are generally modest and site-specific, so it’s normal to see different responses at different skeletal sites (even with the same program)
- Combined impact and resistance training appears most effective
- Longer-duration studies show clearer benefits than short-term trials
Menopausal symptoms:
- Exercise significantly reduces insomnia severity, particularly in women with baseline sleep problems
- Mood and quality of life generally improve with regular exercise
- Evidence for reducing hot flash frequency is inconsistent. Some women report improvement, but rigorous reviews find no clear effect
One key detail: During perimenopause itself (while still in transition), short-term exercise studies often show limited changes in bone density and lean mass, while benefits become clearer in early postmenopause with consistent training. This doesn't mean the training "isn't working." It often means you're playing the long game.
Practical recommendations¶
These recommendations can look like a lot on paper, so keep this in mind: you don’t have to change everything at once. Start with the highest-impact moves for your client, build consistency, and then layer in the rest over time. (Progress beats perfection.)
Resistance training:
- Frequency: 2-4 sessions per week, hitting all major muscle groups across the week
- Exercise selection: Compound movements (squats, deadlifts, rows, presses, lunges) form the foundation because they load multiple joints, stimulate more total muscle mass, and carry over well to daily life
- Progressive overload is essential: Gradually increase challenge over time (add weight, add reps, add sets), because without progressive challenge, muscles don’t adapt
- Volume considerations: Research suggests postmenopausal women may need higher training volumes (more total sets per muscle group) to achieve muscle growth compared to premenopausal women; in practice, that means you don’t need to be afraid of programming substantial training when recovery supports it
- Intensity matters: Lifting heavy (relative to the individual) provides more stimulus for muscle and bone than high-rep, low-weight approaches. Help clients understand that “heavy” is personal, meaning it should feel appropriately challenging for them
- Recovery: Sleep disruption can impair recovery, so you may need to adjust session frequency or intensity during periods of poor sleep. (This is common, and it’s workable.)
- Focus on strength and function: Frame the goal as getting stronger and more capable, not just “toning.” Strength is protective and functional
Impact loading for bones:
- Include jumping, hopping, or skipping if appropriate for the client, since these activities provide mechanical loading that stimulates bone remodeling
- Even brief impact sessions provide bone stimulus, so this doesn’t need to be lengthy
- Progress gradually while considering joint health and current fitness level
- For clients with osteoporosis or joint issues, modify or substitute with resistance training
- Examples: jump rope, box step-ups with emphasis on the step-down, low hurdle hops, lateral bounds
- Meta-analyses show mixed-loading programs (combining impact with resistance training) are most effective for preserving bone at the hip and spine
- Start conservatively: 10-20 jumps per session is a reasonable starting point for someone new to impact training
Aerobic training:
- Include aerobic training for cardiovascular health and fat mass management
- Zone 2 (conversational pace) training 150+ minutes weekly is a solid foundation
- It can be combined with resistance training in the same program
- Since cardiovascular risk increases after menopause, aerobic fitness often becomes more important over time
- Walking is effective and sustainable for many women
- Higher intensities (interval training) may provide additional metabolic benefits, but it helps to balance them with recovery needs (especially if sleep is a bit messy)
- Swimming and cycling are joint-friendly options for women with joint concerns
Balance and stability:
- Falls become a greater concern as women age, and fall-related fractures are a serious consequence of poor bone health
- Include balance challenges and single-leg work in programs, especially for clients with bone density concerns
- Progress from stable to unstable surfaces, and from bilateral to unilateral exercises
- Functional movements like getting up from the floor, stepping over obstacles, and carrying loads while moving all challenge balance in practical ways
- Consider yoga, Tai Chi, or dedicated balance work as adjuncts to strength training
A brief note on cycle-based training¶
For perimenopausal clients who still have menstrual cycles, you may have heard about “cycle-based training,” where training intensity is adjusted based on menstrual cycle phase.
Some research in young, regularly cycling women suggests:
- The follicular phase (early cycle) may support higher intensity training
- The luteal phase (later cycle) may warrant adjusted intensity if symptoms or recovery are affected
For your perimenopausal clients:
- Cycles are often irregular during perimenopause
- Individual variation is enormous (so what works for one person might be a mismatch for another)
- A pragmatic approach: encourage clients to notice their own patterns and adjust if needed
- Avoid rigid protocols, and listen to the client
For postmenopausal clients, cycle-based considerations don’t apply since menstrual cycles have stopped.
Common training mistakes¶
The longevity protocol identifies common mistakes women make during this transition. Another way to think about these is "common pitfalls," especially when someone is doing their best but working with a changing body.
- Avoiding heavy weights: Many women shy away from lifting heavy, which means they miss the stimulus needed for bone and muscle maintenance
- Excessive cardio without strength training: Cardio alone won’t preserve muscle or stimulate bone
- Not adjusting for hormonal changes: Ignoring recovery needs or symptom impacts can backfire, even when motivation is high
- Under-recovering: Not accounting for the sleep disruption that often accompanies menopause
- All-or-nothing thinking: Abandoning exercise entirely when symptoms are challenging
If a client recognizes themselves in any of these, that’s okay. It’s common, and it gives you a clear place to start coaching. (Awareness is progress.)
Coaching in practice: When cardio "stops working"¶
The scenario: A client in her late 40s or 50s says, "I've been doing my usual cardio but it's just not working anymore. I'm gaining weight around my middle and I feel weaker."
What NOT to do:
❌ Tell her that cardio is now "useless" or insist she just needs to eat less and work harder.
Why it doesn't work: It dismisses her experience, oversimplifies what's happening physiologically, and can create shame or all-or-nothing thinking.
What TO do:
✅ Validate her frustration, explain what's changing in clear language, and position strength training as an important addition (not a replacement) for her cardio.
Sample dialogue:
Client: "I've been doing my usual cardio but it's just not working anymore. I'm gaining weight around my middle and I feel weaker."
Coach: "That's really common during menopause, and it can be incredibly frustrating. You're putting in the effort and not getting the same return."
Client: "Exactly. It makes me wonder why I bother."
Coach: "What we see around this stage of life is that as estrogen drops, your body tends to shift where it stores fat, and you lose muscle faster than before. Cardio is still great for your heart and overall health, but it doesn't give your muscles or bones the kind of challenge they need to stay strong."
Client: "So what should I do? Stop cardio?"
Coach: "You don't have to stop at all. I'd suggest we add strength training: real resistance work, not just light weights. Your body needs that stimulus to maintain muscle and keep bones strong. We can keep some cardio for heart health and add two or three strength sessions a week, starting right where you are and building gradually. How does that sound?"
Client: "That actually feels doable. I'd like to feel strong again."
[CHONK: Nutrition for Female Hormonal Health]
Nutrition during the menopause transition¶
Nutrition plays a supporting role during menopause. It won't make symptoms disappear, but it can help you preserve muscle, support bone health, and influence how body composition changes over time.
And if you’re thinking, “So I still might have symptoms even if I eat perfectly?” Yep. That’s normal, and it’s not a personal failure.
Protein: More important than ever¶
As women age and estrogen declines, the body can become more "anabolic resistant," which basically means it takes a stronger protein signal to stimulate muscle protein synthesis. So the protein amount that worked great in your 30s may not hit the same way in your 50s.
Targets:
- Aim for 1.0-1.2 grams of protein per kilogram of body weight daily (some evidence suggests up to 1.6 g/kg for active individuals)
- Distribute that protein across meals (about 25-35 grams per meal), particularly if muscle preservation is a priority; research also shows women consuming higher protein intakes have better physical function and higher relative muscle mass
Practical strategies to increase protein:
- Prioritize protein at each meal by making it the anchor of the plate, and include protein-rich snacks if needed to meet targets (Greek yogurt, cottage cheese, jerky, hard-boiled eggs)
- Consider spreading protein throughout the day rather than loading most of it at dinner, and track for a few days as a reality check, since many people (very understandably) overestimate their protein intake
Practical note: One of the most common mistakes women make during menopause is under-eating protein. A client doing great on 0.8 g/kg in her 30s may need more in her 50s, so don’t assume her current intake is adequate. Take a minute to actually calculate it with her (or for yourself) to be sure. (This is one of those tiny steps that can make a big difference.)
| For DIY Learners |
|---|
| Applying this to yourself: Do you actually know how much protein you’re eating daily? Most people overestimate. Try tracking for 3-4 days (honestly, including the days when meals are less structured). If you’re a woman over 40, the target is 1.0-1.2 g/kg body weight, potentially more if you’re very active. For a 150-pound (68 kg) woman, that’s 68-82 grams of protein per day minimum. Are you hitting that? And importantly, is it distributed across meals, or are you cramming most of it at dinner? Small shifts here (a Greek yogurt at breakfast, cottage cheese as a snack) can make a meaningful difference in muscle preservation. |
Bone health nutrition¶
Bone health can feel like a “future me” problem until it suddenly isn’t, so it’s worth building a few simple habits now. (No perfection required.)
Calcium:
- Target: approximately 1000-1200 mg daily from food and supplements combined, using food sources like dairy, fortified plant milks, canned fish with bones, leafy greens, and tofu
- If supplementing, split doses (≤500-600 mg at a time) to improve absorption, and avoid very high supplemental calcium doses, which may carry cardiovascular concerns
Vitamin D:
- Essential for calcium absorption and bone health
- Many postmenopausal women have insufficient vitamin D
- Target: 800-2000 IU daily, depending on blood levels and sun exposure
- Important to ensure sufficiency before or alongside any osteoporosis treatment
Vitamin K2:
- Plays a role in directing calcium to bones
- Found in fermented foods, some cheeses, and egg yolks
- Often included in bone health supplements
Body composition challenges¶
Women often experience frustrating body composition changes during menopause. Weight gain, particularly around the abdomen, can happen even when eating and exercise habits haven’t changed, which can feel confusing and unfair. (You’re not imagining it.)
What’s happening:
- Hormonal shifts can favor central fat storage, while lean mass decline can reduce metabolic rate
- Sleep disruption can affect appetite hormones, and stress and life circumstances often peak during midlife
Evidence-based approach:
- Focus on body composition, not just scale weight. The scale may not move much even as body composition improves
- Preserve muscle through resistance training and protein (this is one of those non-negotiables, even if it’s not the answer anyone hopes for)
- Moderate calorie reduction if needed (500-750 kcal/day deficit); guidelines suggest targeting 5-10 percent weight loss over about 6 months
- Avoid very low calorie diets that sacrifice muscle. Muscle loss worsens the underlying metabolic challenges
- Set realistic expectations. Slow, sustainable change beats rapid weight cycling
- Consider that some body composition change is normal and not entirely preventable
The protein leverage hypothesis suggests that when protein intake is inadequate, the body may drive overconsumption of fats and carbohydrates to meet protein needs. Adequate protein may help with appetite regulation, which is another reason protein is often the first priority. (And yes, “protein leverage hypothesis” is the established name for this idea in the research.)
What to tell clients about weight changes:
Many women feel they’re “doing everything right” but gaining weight. Validate this frustration, because it’s real, and then help them zoom out to what’s actually in their control:
- Some change is hormonal and not fully controllable through diet and exercise, and body composition often matters more than scale weight
- Maintaining current weight while improving body composition is a win, and the goal is long-term metabolic health, not short-term scale victories
If a client feels discouraged here, that’s OK. This stage can require a mindset shift as much as it requires a nutrition plan, and it can take a little time to make peace with what “progress” looks like now. (Totally normal.)
Iron considerations¶
An interesting shift happens after menopause: iron needs decrease once menstrual bleeding stops. If this surprises someone, you’re not alone. (It’s a common point of confusion.)
- Premenopausal women need more iron due to menstrual losses, while postmenopausal women’s iron needs drop to the same level as men
- Iron supplementation is rarely needed after menopause unless testing shows deficiency, and excess iron can be harmful, so don’t supplement without testing
Other key nutrients¶
These aren’t “magic,” but they can support the basics like bone, sleep, muscle function, and heart health. (Which adds up.)
Magnesium:
- Supports bone health, sleep, and muscle function, and many women don’t meet recommendations
- Food sources include nuts, seeds, whole grains, and leafy greens
Omega-3 fatty acids:
- Support cardiovascular health and may have anti-inflammatory effects; found in fatty fish, walnuts, and flaxseeds
- Supplementation of 2-3 g EPA/DHA daily is often recommended for those who don’t eat fish regularly
Time-restricted eating considerations¶
Some women find time-restricted eating (TRE) helpful for weight management. During menopause, though, it’s smart to treat it like an experiment and pay attention to how you respond. (Spoiler: there’s no one “right” window.)
- Ensure protein targets are met within the eating window, and avoid aggressive fasting that could compromise muscle
- If trying TRE, monitor how you feel (some women find symptoms, particularly sleep or mood, worsen with extended fasting) and adjust accordingly; 12-14 hour overnight fasts are generally gentler than longer windows
A note on phytoestrogens¶
Phytoestrogens (plant compounds with weak estrogen-like activity found in soy, flaxseeds, and other foods) are sometimes promoted for menopause symptoms.
What the evidence shows:
- A Cochrane review found no significant benefit over placebo for hot flashes, and effects, if any, appear small
- Some mechanistic research suggests potential benefits for bone and metabolic health
- Generally safe as part of a balanced diet, but not a replacement for medical treatment when symptoms are significant
If someone was really hoping soy or flax would be a straightforward fix for hot flashes, it makes sense to feel disappointed. The upside is that these foods can still fit nicely into a balanced diet for overall health.
Coaching in practice: Addressing weight gain concerns¶
The scenario: A client says, “I’m doing everything the same as I used to and I just keep gaining weight. Nothing works anymore.”
What NOT to do:
❌ Assume she’s “cheating” on her plan, or tell her she just needs to try a very low calorie diet or do even more cardio.
Why it doesn’t work: It ignores the real physiological changes of menopause, increases shame, and often leads to unsustainable, all-or-nothing efforts.
What TO do:
✅ Validate her experience, explain what’s changing, and focus on protein, strength training, and realistic expectations about the pace and extent of change.
Sample dialogue:
Client: “I’m doing everything the same as I used to and I just keep gaining weight. Nothing works anymore.”
Coach: “I hear you. That’s one of the most frustrating parts of this stage of life. You’re putting in effort, and your body isn’t responding the way it used to.”
Client: “Exactly. It makes me feel like my body is broken.”
Coach: “Your body isn’t broken, but it is changing how it processes and stores energy. Hormonal shifts around menopause tend to favor more fat around the abdomen, and at the same time, most women lose muscle, which can lower metabolic rate. On top of that, sleep and stress can shift appetite and cravings. So you’re not imagining this.”
Client: “So is there anything I can actually do?”
Coach: “There are a few things that can genuinely help, even if they don’t make the scale behave exactly like it did in your 30s. First, we make sure you’re getting enough protein, because that’s the number one thing I see women under-do. Second, strength training becomes even more important to maintain muscle and metabolism. Third, we work on expectations: the scale might move more slowly than it used to, but we can absolutely improve your body composition and how you feel in your body.”
Client: “That feels more realistic. Where should we start?”
Coach: “Let’s pick one place that feels doable, maybe adding a bit more protein to breakfast, or starting two short strength sessions per week. We can build from there and adjust based on how your body responds.”
[CHONK: Coaching Women Through Hormonal Transitions]
Staying in scope while providing real support¶
Welcome to the point where everything starts to click: you’ve got the physiology down, you understand the context around HRT, and you have smart training and nutrition strategies to draw on.
Now comes the practical question: How do you coach effectively while staying firmly within scope?
If that tension feels tricky to navigate, that’s normal. With practice, it starts to feel more natural.
What coaches CAN do¶
Think of this as your “high-impact, clearly in-scope” zone.
Education and information:
- Explain what happens during the menopause transition in general terms, and remind clients that it’s a biological shift rather than a disease or personal failure.
- Share that there’s evidence for a range of interventions, and help clients come up with questions to bring to their healthcare provider.
Lifestyle support:
- Design training programs and provide nutrition guidance within scope, then adjust based on symptoms and recovery, since recovery often changes in midlife.
- Support sleep hygiene and stress management strategies so the plan stays doable in real life.
Care navigation:
- Encourage conversations with healthcare providers, including whether a specialist consultation might be helpful.
- Help clients prepare for medical appointments so they feel less rushed and more confident, then support implementation of medical recommendations.
Emotional support:
- Listen without judgment, validate the challenges of this transition, and provide consistency and encouragement over time.
- Help clients maintain perspective, especially on the hard days, without minimizing what they’re experiencing.
In practice, it can sound like:
Client: “Is this normal, or is something wrong with me?”
Coach: “A lot of these symptoms are common in the menopause transition, and you’re not doing anything ‘wrong.’ I can help with training, nutrition, sleep, and stress, and we can also make a list of questions for your clinician so you feel supported on both sides.”
What coaches CANNOT do¶
This is where staying in scope protects your client and protects you.
Medical practice:
- Diagnose conditions (including menopause itself), interpret lab results, or tell a client what their results “mean” for their treatment.
- Recommend for or against HRT, suggest specific medications, formulations, or doses, or advise on starting, stopping, or adjusting medical treatments.
Testing interpretation:
- You can explain what common hormone tests measure in general terms, but interpretation belongs to the client’s healthcare provider.
In practice, it can sound like:
Client: “Should I increase my dose?”
Coach: “That’s a great question for your prescriber, because it depends on your health history and symptoms. What I can do is adjust your training and recovery plan based on how you’re feeling day to day.”
When to refer¶
Some situations call for medical support, and that doesn’t mean your client is “broken.” It just means the right next step is a clinician’s assessment, and your coaching still matters alongside that.
These situations warrant medical referral:
Urgent (immediate medical attention):
- Any vaginal bleeding after menopause (postmenopausal bleeding is a red flag)
- Severe or worsening pelvic pain, especially with fever, or other signs of serious illness
Prompt medical consultation:
- Symptoms significantly affecting quality of life (hot flashes disrupting sleep night after night, mood changes interfering with relationships or work)
- Symptoms not responding to lifestyle measures after a reasonable trial
- Client interested in discussing HRT or other medical treatments
- Suspected premature menopause (before age 40). These clients need specialist evaluation
- History of hormone-sensitive cancers, blood clots, or significant cardiovascular disease, or other complex medical conditions affecting lifestyle recommendations (complex medical decision-making required)
- Concerning bone density results (osteopenia or osteoporosis)
- Depression or anxiety that's more than mild or situational (screen for mental health needs), genitourinary symptoms causing significant distress (vaginal therapies may help), or persistent bleeding irregularities that haven't been evaluated
If the referral list feels a little intense, you don’t need to memorize it. You just need to recognize when something is outside coaching scope and help your client get appropriate care.
What to say:
Client: "I’m not sure if this is just menopause, but it’s starting to feel like too much."
Coach: "What you're describing sounds like something worth discussing with your doctor. They can evaluate whether there are medical options that might help. I’m here to support you with the lifestyle side, but this is beyond what I can address as a coach."
Supporting clients on HRT¶
Some of your clients will be taking HRT, and your job isn’t to be “pro-HRT” or “anti-HRT.” Your job is to coach the human in front of you.
Do:
- Keep coaching the lifestyle basics that matter regardless of HRT status, including nutrition, training, recovery, and sleep.
- Check in on how they're doing overall, and adjust training if they mention side effects that affect workouts or recovery.
Don't:
- Comment on whether they should be on HRT, or express skepticism or enthusiasm about their medical treatment.
- Offer opinions about their formulation or dose, or suggest changes to their HRT.
In practice, it can sound like:
Client: “I started HRT last month and I’m not sure how to train right now.”
Coach: “Thanks for telling me. I can’t weigh in on the medication side, but I can help you adjust your workouts and recovery based on how your energy, sleep, and symptoms are showing up this week.”
Your role is the same as with any client on medication: support lifestyle factors and stay in your lane. Simple on paper, not always easy in practice.
Supporting clients not on HRT¶
Some clients will choose not to use HRT, or it may not be appropriate for them. They deserve the same steady support and respect.
Do:
- Respect their decision and focus on lifestyle factors that can help, like strength training, sleep support, and nutrition basics.
- Maintain realistic expectations: lifestyle can help but may not eliminate symptoms, and some discomfort may persist without anyone doing it “wrong.”
Don't:
- Push them toward HRT or imply they're "missing out."
- Guarantee that lifestyle changes will resolve their symptoms.
In practice, it can sound like:
Client: “I don’t want HRT, but I still want to feel better.”
Coach: “That makes sense. We’ll work with what’s in your control, and we’ll aim for noticeable improvement, even if we can’t promise every symptom disappears.”
Managing expectations¶
Honest expectation-setting is one of the most valuable things you can offer, and it’s also one of the hardest, because you want your client to feel better fast.
Instead of treating menopause like something to “fix,” help clients plan for a normal transition where progress can look different than it did at 25. That usually includes accepting that some symptoms may linger despite best efforts, focusing on thriving in a changing body (not returning to “before”), and prioritizing consistency over perfection, every time.
In practice, it can sound like:
Client: “I’m doing everything right. Why do I still feel off?”
Coach: “I get why that’s discouraging. You’re doing a lot of the right things, and it may still take time. Let’s focus on the habits that move the needle most, and we’ll track progress in a way that fits what your body is doing right now.”
Deep Health integration¶
Menopause can touch every dimension of Deep Health:
| Dimension | Consideration |
|---|---|
| Physical | Managing symptoms, body composition changes, bone health, and cardiovascular risk |
| Emotional | Mood shifts, identity changes, and frustration with body changes |
| Mental | “Brain fog,” confidence changes, and shifts in self-perception |
| Environmental | Sleep setup and practical temperature management, especially for night sweats |
| Relational | Impact on relationships, communication with partners, and changing family roles |
| Existential | Life transitions, meaning-making, and “who am I now?” questions |
So if a client is struggling with menopause symptoms, they may also be juggling aging parents, kids leaving home, career shifts, and relationship changes. In other words, the physical symptoms are happening inside a whole life, and that context matters.
How Deep Health informs your coaching:
Physical: This is your primary domain. Training, nutrition, sleep hygiene, and movement all fall within coaching scope.
Emotional: Validate feelings, because mood changes are real and can be partly hormonal. You can support coping strategies and stress management; if what you’re hearing suggests clinical depression or anxiety, refer to mental health professionals.
Mental: “Brain fog” is frustrating, but it usually resolves. You can reassure clients that cognitive function typically remains within normal limits, while also supporting the basics that influence cognition, especially sleep and stress management.
Environmental: Help with practical adjustments, such as setting up a sleep environment for night sweats, using temperature control strategies, and ensuring access to movement opportunities.
Relational: Acknowledge that relationships may be affected and encourage communication with partners. Also recognize that midlife often includes caregiving responsibilities, which can change time, energy, and bandwidth.
Existential: Menopause often coincides with bigger questions, such as: "What do I want from this next phase of life?" You can create space for these conversations without providing therapy, and you can help clients connect their health behaviors to their larger values and goals.
You're not meant to "fix" every dimension; you're meant to notice what's there and coach within scope.
The midlife context¶
One important thing to keep in mind is that menopause doesn't happen in isolation. This life stage often brings:
- Family shifts, like children leaving home (or returning), which can change routines and roles.
- Caregiving demands, including aging parents who need more time, energy, and attention.
- Work and relationship transitions, from peak career demands to divorce, loss, or “empty nest” adjustments.
- Other health and life pressures, including family health concerns and financial stress around college or retirement.
If you're reading this and thinking, "No wonder my clients feel overwhelmed," that’s a completely normal reaction. It’s a lot to carry.
All of these stressors affect hormones, sleep, eating, and exercise adherence. A coaching approach that only addresses physical symptoms misses the larger picture. This is exactly why the Deep Health model matters: it helps you see your client's full context.
Coaching in practice: Supporting a client through early menopause¶
The scenario: Sarah, 48, reports that her periods have become irregular over the past year. She's experiencing hot flashes (4-5 per day), sleep disruption (waking 2-3 times nightly), and has gained about 8 pounds despite no changes in eating. She says she feels "foggy" and has less energy than she used to. She's frustrated and says she "feels like she's falling apart."
Sarah asks if she should try HRT.
What NOT to do:
❌ Tell her, "This is definitely perimenopause; you should go on HRT" or suggest specific hormones or doses.
Why it doesn't work: That crosses into diagnosis and medical prescribing, which are outside your scope, and it oversimplifies what might be going on.
What TO do:
✅ Validate her experience, acknowledge that her symptoms are common in the menopause transition, be clear about your scope boundaries, encourage medical evaluation, and offer concrete lifestyle support.
Sample dialogue:
Sarah: "My periods are all over the place, I'm having hot flashes all day and night, I've gained eight pounds without changing anything, and I feel foggy all the time. I honestly feel like I'm falling apart. Do you think I should try HRT?"
Coach: "I can hear how overwhelming this feels, and it makes sense you'd be frustrated. A lot of what you're describing, like irregular periods, hot flashes, sleep disruption, weight changes, and brain fog, is really common during the transition into menopause. That doesn’t make it easy, but it does mean you’re not alone in this."
Sarah: "It's almost a relief to hear that, but I still don't know what to do."
Coach: "Totally understandable. About HRT specifically, that’s something I can’t advise you on. It’s a medical decision that depends on your individual health history and risk factors, so I’d encourage you to talk with your doctor or a menopause specialist who can help you understand your options."
Sarah: "Okay, I can do that, but I also just want to feel better day to day."
Coach: "Absolutely, and we can work on that. What I can do is support the lifestyle pieces that genuinely help during this transition, such as your sleep environment and habits, nutrition (especially making sure you’re getting enough protein), and an exercise approach that supports you instead of draining you. These won’t necessarily eliminate every symptom, but they can make a real difference in how you feel."
Sarah: "That sounds helpful. Where should we start?"
Coach: "How about we start by looking at your sleep and recovery? If we can get you sleeping a bit better, that often helps with mood, energy, and even appetite. We’ll work on that while you’re having the medical conversation, too."
Key elements:
- Validated her experience and normalized common symptoms, without diagnosing her.
- Stayed clear on scope boundaries, while still offering concrete support and direction.
- Encouraged medical consultation, and avoided commenting on specific medications, doses, or changes.
Common Mistakes to Avoid: Coaching Women Through Midlife¶
You’ll see a few common patterns during perimenopause and menopause. None of these are “bad client behavior.” They’re understandable habits and beliefs that just need an update for this stage of life, and you can help with that.
Here are mistakes to watch for and help clients address:
Under-eating protein. This is extremely common. Many women in midlife are still eating the same modest protein portions they always have, but their bodies now need more to maintain muscle mass. Help clients aim for 30+ grams per meal and understand why protein needs increase with age and declining estrogen.
Under-eating fiber. Fiber supports gut health, blood sugar regulation, and satiety, all of which become more important during hormonal transitions. Many women don't hit the 25-30+ grams daily target.
Avoiding heavy weights. Fear of "bulking up" leads many women to stick with light weights or cardio only. The reality: heavy resistance training is one of the most protective interventions for bone density, muscle mass, and metabolic health during and after menopause. Help clients understand that heavy weights don't cause bulkiness; they build strength and protect against age-related decline.
Ignoring iron status. During perimenopause, heavy or irregular periods can cause iron deficiency that contributes to fatigue. After menopause, iron needs decrease and excess iron can be problematic. Encourage clients to work with their doctors to monitor iron status appropriately for their stage.
Not adjusting for hormonal changes. Training intensity, recovery needs, sleep strategies, and nutrition all may need adjustment during hormonal transitions. Clients who try to "push through" without modifications often end up exhausted or injured. Help them listen to their bodies and adapt.
Excessive cardio without strength training. Some women respond to weight changes by adding more cardio, which can actually accelerate muscle loss. The evidence strongly supports prioritizing resistance training during and after menopause, with cardio as a complement rather than the main focus.
Understanding these patterns helps you proactively guide clients away from common pitfalls and toward strategies that actually support them during this transition.
[CHONK: Study Guide Questions]
Study guide questions¶
These questions help you work through the material and prepare for the chapter exam. They're optional, but answering even a few can help reinforce what you’re learning. If you’re short on time, pick the ones that feel most relevant, and aim for clear, client-friendly answers rather than “perfect” ones.
-
What is the difference between perimenopause and menopause, and why does that distinction matter for coaching?
-
If a client asks about hormone replacement therapy (HRT), such as "Is HRT safe?", how would you respond in a way that's informative but stays within scope?
-
Why might postmenopausal women need higher resistance training volumes than premenopausal women to achieve the same muscle-building response?
-
What are three red flags that would prompt you to refer a menopausal client for immediate medical attention?
-
How would you explain to a client why protein needs increase during menopause?
-
A client is frustrated that her cardio routine isn't preventing weight gain like it used to. What would you explain, and what would you suggest?
Self-reflection questions:
These are just for you. A quick, honest check-in is more useful than an “ideal” answer.
-
If you're a woman approaching or in menopause, how much strength training are you currently doing, and does it match the recommendations in this chapter?
-
Regardless of your gender, how can understanding hormonal transitions help you be a more empathetic and effective coach, or advocate for the women in your life?
[CHONK: Works Cited]
Works Cited¶
References¶
These sources support the material covered in this chapter.
-
Office on Women's Health. Menopause basics, U.S. Department of Health & Human Services; 2025. https://womenshealth.gov/menopause/menopause-basics
-
Wegrzynowicz AK, Walls AC, Godfrey M, Beckley A. Insights into Perimenopause: A Survey of Perceptions, Opinions on Treatment, and Potential Approaches. Women, 2025;5(1):4. doi:10.3390/women5010004
-
DELAMATER L, SANTORO N. Management of the Perimenopause. Clinical Obstetrics & Gynecology, 2018;61(3):419-432. doi:10.1097/grf.0000000000000389
-
Paramsothy P, Harlow SD, Nan B, Greendale GA, Santoro N, Crawford SL, et al. Duration of the menopausal transition is longer in women with young age at onset: the multiethnic Study of Women's Health Across the Nation. Menopause, 2017;24(2):142-149. doi:10.1097/gme.0000000000000736
-
Todorova L, Bonassi R, Guerrero Carreño FJ, Hirschberg AL, Yuksel N, Rea C, et al. Prevalence and impact of vasomotor symptoms due to menopause among women in Brazil, Canada, Mexico, and Nordic Europe: a cross-sectional survey. Menopause, 2023;30(12):1179-1189. doi:10.1097/gme.0000000000002265
-
Baker FC, Lampio L, Saaresranta T, Polo-Kantola P. Sleep and Sleep Disorders in the Menopausal Transition. Sleep Medicine Clinics, 2018;13(3):443-456. doi:10.1016/j.jsmc.2018.04.011
-
Salari N, Hasheminezhad R, Hosseinian-Far A, Rasoulpoor S, Assefi M, Nankali S, et al. Global prevalence of sleep disorders during menopause: a meta-analysis. Sleep and Breathing, 2023;27(5):1883-1897. doi:10.1007/s11325-023-02793-5
-
Conde DM, Verdade RC, Valadares ALR, Mella LFB, Pedro AO, Costa-Paiva L. Menopause and cognitive impairment: A narrative review of current knowledge. World Journal of Psychiatry, 2021;11(8):412-428. doi:10.5498/wjp.v11.i8.412
-
Nair AR, Pillai AJ, Nair N. Cardiovascular Changes in Menopause. Current Cardiology Reviews, 2021;17(4). doi:10.2174/1573403x16666201106141811
-
Rani J, Swati S, Meeta M, Singh SH, Tanvir T, Madan A. Postmenopausal Osteoporosis: Menopause Hormone Therapy and Selective Estrogen Receptor Modulators. Indian Journal of Orthopaedics, 2023;57(S1):105-114. doi:10.1007/s43465-023-01071-6
-
Nudy M, Chinchilli VM, Foy AJ. A systematic review and meta-regression analysis to examine the ‘timing hypothesis’ of hormone replacement therapy on mortality, coronary heart disease, and stroke. IJC Heart & Vasculature, 2019;22:123-131. doi:10.1016/j.ijcha.2019.01.001
-
The North American Menopause Society. The 2022 Hormone Therapy Position Statement, Menopause; 2022. https://pubmed.ncbi.nlm.nih.gov/35797481/
-
Abenhaim HA, Suissa S, Azoulay L, Spence AR, Czuzoj-Shulman N, Tulandi T. Menopausal Hormone Therapy Formulation and Breast Cancer Risk. Obstetrics & Gynecology, 2022;139(6):1103-1111. doi:10.1097/aog.0000000000004723
-
Asi N, Mohammed K, Haydour Q, Gionfriddo MR, Vargas OLM, Prokop LJ, et al. Progesterone vs. synthetic progestins and the risk of breast cancer: a systematic review and meta-analysis. Systematic Reviews, 2016;5(1). doi:10.1186/s13643-016-0294-5
-
Oliveira GMMd, Almeida MCCd, Arcelus CMA, Espíndola L, Rivera MAM, Silva-Filho ALd, et al. Brazilian Guideline on Menopausal Cardiovascular Health – 2024. Revista Brasileira de Ginecologia e Obstetrícia, 2024;46. doi:10.61622/rbgo/2024rbgo100
-
Agostini D, Donati Zeppa S, Lucertini F, Annibalini G, Gervasi M, Ferri Marini C, et al. Muscle and Bone Health in Postmenopausal Women: Role of Protein and Vitamin D Supplementation Combined with Exercise Training. Nutrients, 2018;10(8):1103. doi:10.3390/nu10081103
-
Whitman PW, Alexander CJ, Kaluta L, Burt LA, Gabel L. Does exercising during peri- or early post-menopause prevent bone and muscle loss: A systematic review. Bone, 2025;201:117650. doi:10.1016/j.bone.2025.117650
-
Khalafi M, Habibi Maleki A, Sakhaei MH, Rosenkranz SK, Pourvaghar MJ, Ehsanifar M, et al. The effects of exercise training on body composition in postmenopausal women: a systematic review and meta-analysis. Frontiers in Endocrinology, 2023;14. doi:10.3389/fendo.2023.1183765
-
Kopp D, et al. Resistance training alters body composition in middle-aged women depending on menopause, BMC Women's Health; 2023. https://bmcwomenshealth.biomedcentral.com/articles/10.1186/s12905-023-02671-y
-
Qian J, Sun S, Wang M, Sun Y, Sun X, Jevitt C, et al. The effect of exercise intervention on improving sleep in menopausal women: a systematic review and meta-analysis. Frontiers in Medicine, 2023;10. doi:10.3389/fmed.2023.1092294
-
Daley A, Stokes-Lampard H, MacArthur C. Exercise for vasomotor menopausal symptoms. Cochrane Database of Systematic Reviews, 2011. doi:10.1002/14651858.cd006108.pub3
-
Nahas PC, Rossato LT, Martins FM, Souza AP, de Branco FMS, Carneiro MAS, et al. Moderate Increase in Protein Intake Promotes a Small Additional Improvement in Functional Capacity, But Not in Muscle Strength and Lean Mass Quality, in Postmenopausal Women Following Resistance Exercise: A Randomized Clinical Trial. Nutrients, 2019;11(6):1323. doi:10.3390/nu11061323
-
Khanal P, He L, Degens H, Stebbings GK, Onambele-Pearson GL, Williams AG, et al. Dietary Protein Requirement Threshold and Micronutrients Profile in Healthy Older Women Based on Relative Skeletal Muscle Mass. Nutrients, 2021;13(9):3076. doi:10.3390/nu13093076
-
Gregson CL, Armstrong DJ, Avgerinou C, Bowden J, Cooper C, Douglas L, et al. The 2024 UK clinical guideline for the prevention and treatment of osteoporosis. Archives of Osteoporosis, 2025;20(1). doi:10.1007/s11657-025-01588-3
-
Korean Society of Menopause. The 2024 Guidelines for Osteoporosis, J Menopausal Med; 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11103071/
-
Lumsden MA, Davies M, Sarri G, for the Guideline Development Group for Menopause: Diagnosis and Management (NICE Clinical Guideline No. 23). Diagnosis and Management of Menopause, JAMA Internal Medicine, 2016;176(8):1205. doi:10.1001/jamainternmed.2016.2761
-
Shokri-Ghadikolaei A, Bakouei F, Delavar MA, Azizi A, Sepidarkish M. Effects of health coaching on menopausal symptoms in postmenopausal and perimenopausal women. Menopause, 2022;29(10):1189-1195. doi:10.1097/gme.0000000000002050
-
Wierman ME, Arlt W, Basson R, Davis SR, Miller KK, Murad MH, et al. Androgen Therapy in Women: A Reappraisal: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 2014;99(10):3489-3510. doi:10.1210/jc.2014-2260
-
Fenton A. Weight, Shape, and Body Composition Changes at Menopause. Journal of Mid-life Health, 2021;12(3):187-192. doi:10.4103/jmh.jmh_123_21