Unit 4: The Practice of Longevity Coaching¶
Chapter 4.22: Integration & Prioritization¶
[CHONK: 1-minute summary]
What you'll learn in this chapter:
- How to apply the "Hierarchy of Longevity Needs" to prioritize interventions for any client
- Why the Adherence Paradox means simpler protocols often win long-term
- How to prevent "majoring in the minor" syndrome in clients seeking longevity coaching
- How to build personalized 12-month coaching roadmaps based on client assessment
- How to use the "Longevity Basics Audit" to identify where each client needs to start
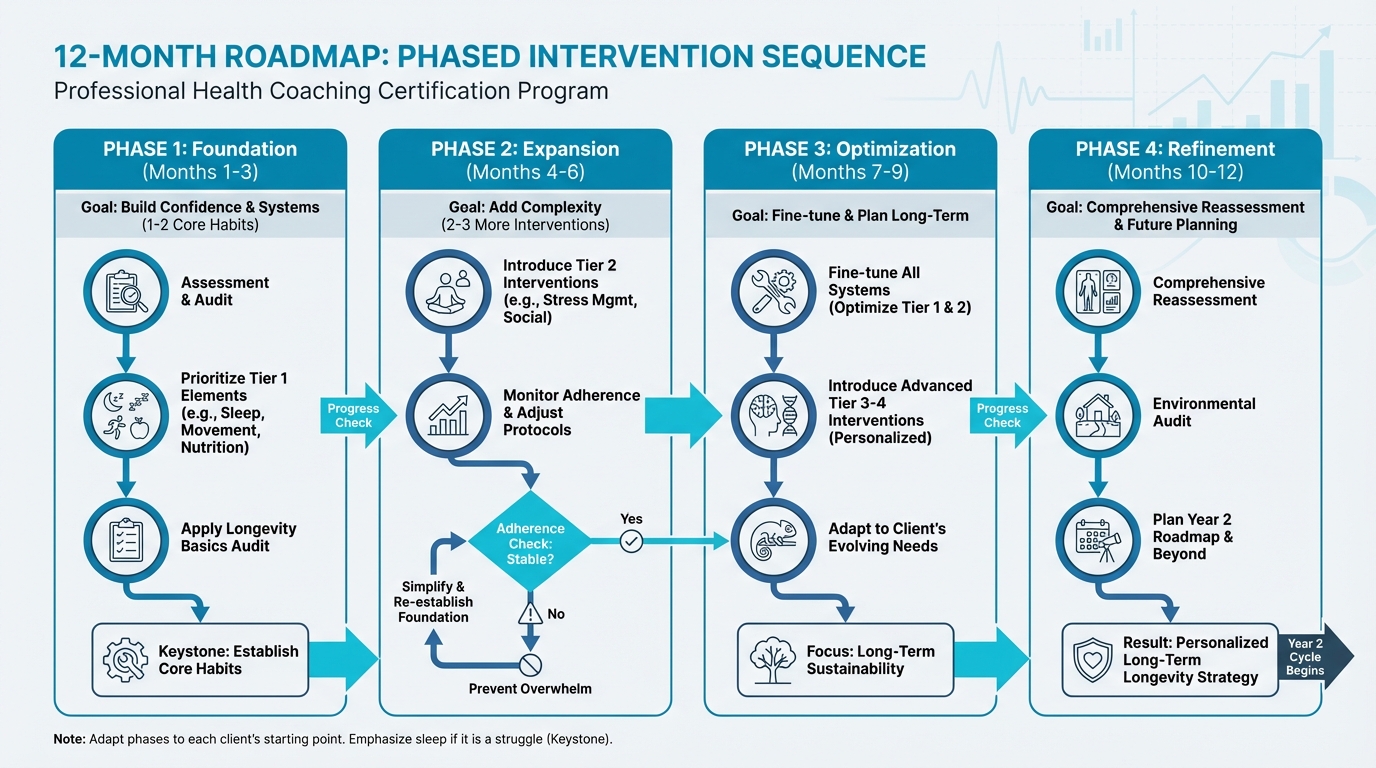
Figure: Phased intervention sequence
The big idea: Your clients have heard about cold plunges, sauna protocols, NMN supplements, and continuous glucose monitors. They've absorbed countless podcast hours on optimization. And many of them are doing all of this while getting five hours of sleep and eating takeout six nights a week. This chapter gives you a structure to help them focus on what actually matters. The interventions with the biggest impact come before chasing marginal gains. The research is clear: 80 percent adherence to a good protocol beats 40 percent adherence to a perfect one. Here's how to put that into practice.
What not to do (example):
Client: "Should I start NMN and cold plunges?"
Coach: "Sure. Let's add a sauna protocol and a CGM, too."
What to do instead (example):
Client: "Should I start NMN and cold plunges?"
Coach: "Maybe later. First, how are you sleeping, and what are you eating most days? Let's start with the basics and make them stick."
[CHONK: Introduction - Don't Biohack Before You Sleep]
Don't Biohack Before You Sleep¶
Picture this client: James is a 45-year-old tech entrepreneur. He takes 23 supplements each morning, owns a $6,000 cold plunge, tracks his glucose continuously, has experimented with rapamycin, and can quote Peter Attia's VO2 max recommendations by heart.
He also sleeps five hours a night, hasn't lifted weights in three years, and his social life consists primarily of Slack messages.
James isn't unusual. He's the archetype of a certain kind of longevity seeker, obsessed with optimizing the margins while the foundation crumbles beneath him.
The Optimization Paradox¶
Here's the uncomfortable truth about longevity optimization: the most exciting interventions are usually the least impactful.
Cold exposure, sauna protocols, exotic supplements, continuous glucose monitoring. These capture attention because they feel high-tech, scientific, controllable. They offer the seductive promise that we can hack our way to a longer life.
But the research tells a different story.
The interventions with the largest effect sizes on mortality and healthspan are the ones your grandmother could have told you about: sleep, movement, eating well, maintaining relationships, not smoking, limiting alcohol. These "boring" basics account for the vast majority of longevity outcomes. Roughly 70 percent or more, according to the best available evidence (1, 2, 3).
Everything else (the biohacks, the supplements, the advanced protocols) falls into the remaining 30 percent, and most of those interventions deliver effects measured in single-digit percentages.
This creates a paradox: clients are drawn to longevity coaching precisely because they want the advanced stuff, but what most of them actually need is help with the basics.
Why This Chapter Matters¶
In Chapter 1.6, you learned the PN 6-step coaching process adapted for longevity and how to assess, understand, strategize, choose, observe, and analyze over multi-year timeframes. You learned about the 3-month phased onboarding and multi-year roadmaps.
This chapter answers a different question: What should you prioritize?
Chapter 1.6 gave you the process. This chapter gives you the hierarchy.
By the end of this chapter, you'll have:
- A clear structure for sequencing interventions (the Hierarchy of Longevity Needs)
- Specific criteria for identifying "Non-Negotiables"
- Tools for recognizing and addressing "majoring in the minor" syndrome
- A practical audit checklist to identify where each client should start
- Coaching language and dialogues for redirecting clients toward what matters
Let's start with the hierarchy.
[CHONK: The Hierarchy of Longevity Needs]
The Hierarchy of Longevity Needs¶
It can help to picture longevity interventions like a pyramid. The base is wide and stable because it’s made up of foundational practices that almost everyone benefits from, and they tend to deliver the biggest effects. As you move up, the pyramid narrows; each level builds on the one below, and each level usually contributes a bit less to overall outcomes. (In other words, most of the payoff comes from the “boring basics,” which is honestly great news.)
The Four Tiers¶
Tier 1 (Foundation): ~70% of outcomes
These are the core essentials, or what you might call the “non-negotiables” for most people. They’re the interventions linked to the largest mortality reductions, and they’re usually the best place to focus first. (Not because anyone is failing if they’re not perfect, but because this is where the biggest return tends to be. We get it.)
- Sleep: 7-9 hours consistently
- Movement: 150+ minutes of physical activity weekly, including strength training
- Basic Nutrition: Adequate protein (target: 30g+ per meal), vegetables, minimally processed foods
- Social Connection: Regular meaningful contact with friends, family, community
- Health Basics: Annual bloodwork, no smoking, alcohol within limits
The effect sizes here are substantial, which is why this tier matters so much. Meeting physical activity guidelines is associated with 20-40 percent reductions in all-cause mortality (4), and each additional 1,000 steps per day is associated with roughly 9 percent lower mortality risk (5). Sleep duration shows up here too: short sleep (under 7 hours) is associated with 14 percent higher mortality, while long sleep (over 9 hours) is associated with 34 percent higher mortality compared to 7-8 hours (6). Social isolation is associated with 32 percent higher mortality, comparable to smoking (7). If all those numbers feel like a lot to keep track of, that’s okay; you don’t need to memorize them. (The takeaway is simpler: these basics move the needle.)
Tier 2 (Significant): ~20% of outcomes
These interventions matter, and they require Tier 1 to be in place first. (Think: add-ons that build a stronger structure, not quick fixes that replace the foundation. And yes, it can be tempting to skip ahead.)
- Stress Management: Structured practices (meditation, breathwork, nature exposure)
- Environment Optimization: Reducing toxin exposure, improving air quality, optimizing light exposure
- Advanced Nutrition: Mediterranean/MIND diet principles, nutrient timing, blood sugar management
Improving diet quality over 12 years is associated with 8-17 percent lower mortality risk, depending on the index used (8). Those gains build on the foundation, though, which means optimizing nutrient timing while sleeping five hours is unlikely to move the needle.
Tier 3 (Minor): ~9% of outcomes
These can be meaningful for clients who already have Tiers 1-2 in a solid place. (If you’re working with someone who loves metrics and “fine tuning,” this is often where they want to play. That’s normal.)
- Supplements: Core supplements (vitamin D, omega-3, magnesium, creatine)
- Recovery Protocols: Sauna, cold exposure, structured recovery
- Testing Optimization: VO2 max testing, biological age clocks, advanced biomarkers
Sauna use (4+ sessions weekly) is associated with roughly 40 percent lower cardiovascular mortality in observational studies (9), but this is in populations who presumably also have other healthy behaviors in place. So these aren’t substitutes for the basics; they’re supports that tend to work best after the basics are working. (Order matters.)
Tier 4 (Marginal): ~1% of outcomes
These are best reserved for clients who truly have everything else dialed in. (And if that’s not your client right now, you’re in very good company.)
- Biohacks: Experimental interventions, precision optimization
- Advanced Testing: Continuous glucose monitoring (for non-diabetics), detailed genetic testing
- Advanced Protocols: Rapamycin, hyperbaric oxygen, peptides
The evidence here is thin, often extrapolated from animal studies or based on mechanistic reasoning rather than human mortality data. For a client who sleeps poorly, these can easily become a distraction from the things that will help most right now. (Spoiler: the basics still win.)
The Graphic: Hierarchy of Longevity Needs¶
If you’re turning this concept into a slide or handout, here’s the straightforward visual spec. (No need to memorize any of this. It’s just to keep the graphic consistent.)
Visual concept: Pyramid structure with 4 tiers, wide at base, narrow at top
Tier 1 (Base - 70% width)
- Label: "Foundation: ~70% of outcomes"
- Color: Deep blue (PN primary #068FB9)
- Contents:
- Sleep (7-9 hours)
- Movement (150+ min/week)
- Basic Nutrition (protein, vegetables)
- Social Connection
- Health Basics (bloodwork, no smoking)
- Tagline: "If you do nothing else, do these"
Tier 2 (Middle-lower - 50% width)
- Label: "Significant: ~20% of outcomes"
- Color: Medium blue (#0D6782)
- Contents:
- Stress Management
- Environment Optimization
- Advanced Nutrition
- Tagline: "Build on the foundation"
Tier 3 (Middle-upper - 30% width)
- Label: "Minor: ~9% of outcomes"
- Color: Light blue (#00bbe3)
- Contents:
- Supplements
- Recovery Protocols (sauna, cold)
- Testing Optimization
- Tagline: "Worth doing after Tiers 1-2 are solid"
Tier 4 (Top - 10% width)
- Label: "Marginal: ~1% of outcomes"
- Color: Lightest blue/gray
- Contents:
- Biohacks
- Experimental Interventions
- Precision Optimization
- Tagline: "For those with everything else dialed in"
Side annotation: Arrow pointing to Tier 3-4 with text "Where many longevity seekers focus" contrasted with "Where most outcomes come from" pointing to Tier 1
Deep Health Across the Hierarchy¶
You can also see how this hierarchy maps to all six Deep Health dimensions:
| Dimension | Tier 1 | Tiers 2-4 |
|---|---|---|
| Physical | Sleep, movement, nutrition | Testing, supplements, recovery |
| Emotional | Social connection | Stress management |
| Mental | Sleep (cognitive function) | Cognitive training, advanced protocols |
| Social | Relationships, community | |
| Environmental | Environment optimization | |
| Existential | Purpose sustaining habits | Long-term planning |
The foundation (Tier 1) touches multiple dimensions simultaneously. Sleep affects physical health, cognitive function, and emotional regulation; social connection supports emotional health and often provides accountability for physical health behaviors; and movement improves mood, cognition, and physical markers.
This is why Tier 1 delivers such outsized returns (which is good news). These interventions create positive cascades across dimensions, so you’re rarely “just” working on sleep or “just” working on movement. If that feels like a lot, you’re not alone. Start with one brick at a time.
[CHONK: The Non-Negotiables]
The Non-Negotiables: What Actually Moves the Needle¶
The longevity protocol (referenced throughout this course) points to six "Non-Negotiables": the interventions with the biggest effects, and the ones worth prioritizing before you chase anything fancy.
If you do nothing else, do these:
- 150 minutes of exercise weekly (strength & cardiovascular)
- Sleep 7-9 hours consistently
- Eat adequate protein (30 grams per meal target)
- Maintain strong relationships/social connections
- Get annual bloodwork
- Don't smoke and avoid excessive drinking
Below is the evidence behind each one, plus how to translate it into coaching.
Exercise: The Most Powerful Longevity Drug¶
Exercise produces larger mortality reductions than any other lifestyle intervention, and possibly larger than most medications.
For example, meeting aerobic activity guidelines (approximately 150 minutes per week of moderate activity) is associated with substantially lower all-cause mortality across ages (4). Even better, the benefits are often greater in older adults than in younger adults, which means it’s never too late to start. (We get it, starting can feel like the hard part.)
One detail that often gets overlooked is that cardiorespiratory fitness is even more predictive than exercise volume alone. High cardiorespiratory fitness is associated with roughly 47 percent lower cancer mortality compared to low fitness (10), and VO2 max is one of the strongest predictors of all-cause mortality we have, outperforming most biomarkers.
What this means for your client: Start with any movement that feels doable, then build from there. Aim for 150 minutes per week as a minimum target, and help clients gradually include both strength training (for muscle mass, bone density, and functional capacity) and cardiovascular training (for VO2 max and metabolic health), because the combination matters.
Sleep: The Foundation of Everything Else¶
Sleep has a U-shaped relationship with mortality, so both short and long sleep are associated with elevated risk.
A 2025 meta-analysis pooling data from 79 prospective cohorts found (6):
- Short sleep (<7 hours): 14 percent higher all-cause mortality
- Long sleep (≥9 hours): 34 percent higher all-cause mortality
- Optimal: 7-8 hours consistently
Sleep also isn’t just about duration. It’s an active metabolic process, and while you’re sleeping, the glymphatic system (the brain’s waste-clearance system) removes beta-amyloid plaques (protein buildups associated with Alzheimer's disease), while growth hormone is released and memory is consolidated, too. (Your body is not “doing nothing” at night.)
What this means for your client: Sleep is foundational because it affects how well every other intervention works. A client who optimizes nutrition but sleeps five hours is fighting with one hand tied behind their back, so it often makes sense to prioritize sleep early in the coaching relationship. If your own sleep isn’t perfect right now, that’s okay; you can work on this alongside your clients.
Nutrition: Adequate Protein and Vegetables¶
Diet quality improvements are associated with meaningful mortality reductions, though the effect sizes are typically smaller than what we see with exercise or sleep.
Improving diet quality over 12 years (measured by validated indices like the AHEI, Alternative Healthy Eating Index, Mediterranean, or DASH score) is associated with 8-17 percent lower all-cause mortality (8). Plant-forward macronutrient profiles are associated with modestly lower mortality, while higher animal fat intake is associated with modestly higher mortality (11).
The key coaching takeaway is this: smaller effect sizes for diet don’t mean nutrition doesn’t matter. They usually mean adequate is more important than optimal for most clients. (And yes, that can feel oddly relieving.)
What this means for your client: Don’t let perfect be the enemy of good. Focus first on adequate protein (30g+ per meal supports muscle protein synthesis), vegetables (6-10 servings daily), minimally processed foods, and limiting alcohol. Once those basics are solid, refinement becomes more valuable. If striving for "perfect" nutrition has ever felt exhausting, you’re not alone; "good enough" really does count here.
Social Connection: As Important as Not Smoking¶
Social connection belongs on this list for a reason. Social isolation is associated with 32 percent higher all-cause mortality, and loneliness is associated with 14 percent higher mortality (7), which puts them in the same ballpark as well-established risk factors like smoking.
Social connection likely works through multiple pathways, including reduced stress, improved immune function, better health behaviors (accountability), and greater meaning and purpose.
What this means for your client: Social connection isn’t a nice-to-have. It’s a Non-Negotiable, and for an isolated client, building connection may be as important as exercise or nutrition. If that feels harder to “prescribe” than a workout plan, you’re not alone. (It’s normal.)
Health Basics: Screening and Harm Reduction¶
Annual bloodwork allows early detection of metabolic dysfunction, inflammation, and disease risk, when problems are often most treatable. This isn’t about optimization; it’s basic prevention.
The harm-reduction basics matter here too. Not smoking produces the largest single-behavior effect on life expectancy (12), and limiting alcohol to 2-4 drinks per week maximum aligns with current evidence on cardiovascular and cancer risk.
What this means for your client: Make sure clients are getting annual bloodwork and stay within scope (Chapter 1.5) when interpreting results. For clients who smoke, cessation may be the single highest-impact intervention, larger than any supplement or biohack.
Coaching in Practice: The Supplement-Obsessed Client¶
[CHONK: Coaching in Practice - The Supplement-Obsessed Client]
The scenario: Your client Marcus, 48, asks about NMN dosing, berberine timing, and whether he should add metformin. He takes 15 supplements daily and spends $400/month on them.
What NOT to do:
❌ Launch into a supplement-by-supplement lecture or design an even more complex stack.
Why it doesn't work: You become a product consultant instead of a coach, and you reinforce the idea that pills matter more than behaviors.
What TO do:
✅ Acknowledge his effort and curiosity, then redirect to the foundations.
Sample dialogue:
Marcus: "I've been reading about NMN and berberine. How much should I take? And do you think I should talk to my doctor about metformin?"
Coach: "You've clearly done a lot of homework, and you're investing a lot in your health. That's impressive." [Pause] "Before we fine-tune your supplement stack, can I ask a few questions about your day-to-day basics?"
Marcus: "Sure."
Coach: "How's your sleep these days?"
Marcus: "Honestly? On a good night, I get five, maybe six hours, but it's all over the place."
Coach: "Got it. And what does a typical week of movement look like?"
Marcus: "I walk the dog and sometimes hike on weekends, but I haven't lifted weights in a while."
Coach: "Thanks for being straight with me. One more: Tell me about your protein intake."
Marcus: "I usually skip breakfast, grab something light for lunch, and then have a big dinner. I have no idea how much protein that adds up to."
Coach: "That helps a lot. Here's what I see: Your interest in supplements shows real commitment, which is great. And the research suggests that sleep and consistent exercise deliver 10–20 times the mortality reduction of even the best supplements. If we can get your sleep closer to 7–8 hours and build a simple strength-training habit, your current supplements will work on a much stronger foundation."
Marcus: "So you're saying I don't have to stop the supplements, but they'd matter more if I fixed the basics first?"
Coach: "Exactly. We can absolutely keep some of what you're doing, and over time we can decide, with your doctor, what really earns its place. For the next month, how would you feel about focusing on sleep and two short strength sessions per week?"
Key takeaway: The goal isn't to dismiss his interests. It's to sequence them appropriately.
The 80/20 of Longevity¶
The Pareto principle (80/20 rule) applies to health interventions. Research on healthcare spending shows that roughly 80 percent of spending is incurred by roughly 20 percent of patients (13). Analysis of global health interventions shows that the top quartile of interventions delivers roughly 79 DALYs (disability-adjusted life years) averted per $1,000, compared to a median of about 5 DALYs/$1,000 (14). In that same analysis, the top ~2.5 percent most cost-effective interventions deliver 25-38 times the median impact.
In practical terms, a small number of interventions deliver the vast majority of results. The Non-Negotiables are those highest-impact interventions for longevity.
[CHONK: Building the 12-Month Roadmap]
Building the 12-Month Roadmap¶
In Chapter 1.6, you learned about the 3-month phased onboarding strategy (Month 1: Foundation, Month 2: Expansion, Month 3: Optimization) and multi-year roadmaps. This section shows you how to apply that approach specifically to the hierarchy of needs.
The Protocol's Phased Approach¶
The longevity protocol recommends building systematically:
Don't try to implement everything at once; build systematically.
Month 1: Foundation
- Sleep optimization; strength training 3x/week; protein targets
- Core supplements (if necessary) and consider HRT (if appropriate)
- Baseline testing (bloodwork, DEXA, VO2 max)
Month 2: Expansion
- Add Zone 2 cardio, and introduce sauna/cold if it fits
- Refine nutrition and stress management practices
- Put extra focus on social connection
Month 3: Optimization
- VO2 max training, plus biomarker testing as appropriate
- Full supplement stack and an environmental audit (as needed)
Ongoing: Refinement
- Quarterly assessments and protocol adjustments
- Continuous education and community building
You'll tailor and simplify this phased plan based on each client's real life.
Adapting the Phases to Each Client¶
These phases are guidelines, not rigid prescriptions. The specifics depend on where each client starts.
If your client already exercises consistently:
- Month 1 might focus on sleep optimization and nutrition refinement, and the foundation phase might be shorter
- You can introduce Zone 2 and strength progression earlier
If your client struggles with sleep:
- Month 1 should heavily emphasize sleep hygiene and consistency, without piling on other interventions that could overwhelm
- Sleep is the keystone, so get this right first
If your client is socially isolated:
- Social connection might be the primary Month 1 focus, alongside a simple physical foundation
- Consider social forms of exercise (group classes, walking partners)
If your client has existing health conditions:
- Coordinate with healthcare providers (scope of practice, Chapter 1.5), prioritize interventions that support medical treatment, and be conservative with adding complexity
Research on Phased vs. All-at-Once Implementation¶
The research generally supports phased approaches, though results vary by context.
A head-to-head trial comparing sequential (one behavior at a time) versus simultaneous (multiple behaviors at once) delivery found (15):
- At 12 months, sequential approaches showed larger overall risk reduction, while at 24 months simultaneous approaches caught up or exceeded
- Sequential approaches achieved higher smoking abstinence at both timepoints
Another trial found that starting with diet could temporarily suppress increases in physical activity, while exercise-first yielded early PA gains (16). By 12 months, all groups improved. The path mattered for early momentum.
Key insight: Phased implementation isn't always superior, but it reduces overwhelm, builds confidence through early wins, and is more sustainable for most clients. The WHO reports that only about 50 percent of patients with chronic conditions adhere to long-term therapies in developed countries (17), which is one reason simpler plans tend to stick.
What this means for your client: Start with 1-2 interventions in Month 1 so they can build confidence and systems before you add complexity. Keep an eye on adherence, and if it starts dropping, it usually means you've added too much too fast.
Coaching in Practice: Sample 12-Month Roadmap¶
What NOT to do (all-at-once overwhelm):
Coach: “Great, so we’re going to fix your sleep, start lifting three days a week, add Zone 2, do sauna and cold, overhaul your diet, add a full supplement stack, and get all your testing done this month.”
Client: “That’s… a lot. I’m not sure where to start.”
Coach: “Just follow the plan. We’ll push through.”
A better approach (phased, client-led):
Coach: “Before we map out the year, can I ask what feels most doable right now: sleep, training, or nutrition?”
Client: “Honestly, sleep. I’m exhausted, and everything else feels harder because of it.”
Coach: “That makes sense. Let’s make Month 1 about a strong foundation: sleep first, plus the minimum effective dose of training and protein so you still get momentum.”
Client: “So we’re not doing everything at once?”
Coach: “No. We’ll earn the right to add more. If your sleep and routines get steadier, Month 2 is where we expand.”
Client: “Okay. What would the first three months look like?”
Coach: “Here’s a simple draft, and we’ll adjust it based on your schedule and what you can actually stick with.
- Month 1 (Foundation): Sleep routine + strength training 3x/week + protein targets; baseline testing if appropriate.
- Month 2 (Expansion): Add Zone 2 cardio; refine nutrition; choose one recovery practice (sauna/cold) if it fits.
- Month 3 (Optimization): VO2 max training; consider more advanced testing and supplements only if the basics are consistent.
Then we reassess each quarter and decide what’s worth adding, changing, or simplifying.”
Client: “How do we know if we’re moving too fast?”
Coach: “If adherence starts slipping for more than a week or two, that’s our signal to scale back and make the plan easier to execute.”
[CHONK: Coaching in Practice - Sample 12-Month Roadmap]
Client profile: Elena is 52 and a busy executive. Right now she’s sleeping about 5-6 hours most nights, exercising sporadically (mostly occasional yoga), and her nutrition is a bit erratic: she often skips breakfast and ends up eating late dinners. Socially, she has a strong family network but limited friendships outside of that. Her VO2 max is 28, which is below the target of 35+.
Month 1: Foundation
- Primary focus: Sleep, aiming for 7 hours with a consistent bedtime (this is the “make everything else easier” move)
- Secondary: Build a daily movement habit with a 10-minute walk most days, ideally at a consistent time
- Assessment: Get baseline bloodwork and establish a Deep Health baseline so you can measure progress
Month 2: Expansion
- Continue sleep optimization and nudge toward 7.5 hours, using the same bedtime routine
- Add strength training 2x/week, focusing on compound movements, good form, and steady progression
- Begin a protein focus by aiming for 30g at breakfast and lunch, then adjust for schedule
Month 3: Optimization
- Maintain the sleep work while continuing strength training
- Add Zone 2 cardio 2x/week, building toward 150 min total
- Refine nutrition using Mediterranean principles (simple, repeatable, and realistic)
Months 4-6: Building
- Progress strength training to 3x/week as recovery and schedule allow
- Increase Zone 2 toward 150+ minutes weekly
- Add a social focus by reconnecting with old friends, starting with 1 coffee date/week
Months 7-9: Deepening
- Introduce stress management practices (start small and pick something she’ll actually do)
- Consider core supplements if gaps exist
- Retest VO2 max, targeting an improvement to 30+
Months 10-12: Refinement
- Fine-tune all systems based on what’s working and what’s getting in the way, keeping the changes small and specific
- Do an environmental audit of her home, office, and schedule to reduce friction
- Plan a Year 2 roadmap that builds on the biggest wins
- Complete a full reassessment (labs, Deep Health, and performance markers)
Coach: "When you look at this as a year-long plan, how does it feel?"
Elena: "Honestly, it feels doable when we break it into chunks like this."
Key takeaway: Notice that sauna, cold exposure, and optimization protocols don't appear until the foundation is solid, if at all in Year 1. Elena's gaps are in Tier 1, so Tier 3 can wait. |
[CHONK: The Adherence Paradox]
The Adherence Paradox¶
Here's the counterintuitive truth at the heart of longevity coaching:
80% adherence to a good protocol beats 40% adherence to a perfect protocol.
This is the Adherence Paradox. The more complex and "optimized" a protocol becomes, the harder it is to sustain, and unsustainable protocols fail, no matter how scientifically sound they are.
Why Simpler Wins Long-Term¶
Cognitive load matters. Tracking 15 supplements, timing meals around workouts, monitoring glucose, optimizing sleep hygiene, maintaining a complex strength program. Each intervention consumes mental bandwidth. Eventually, something gives.
A 2021 study found that overly customized feedback in a physical activity app actually reduced user engagement. More personalization wasn't better (18). There's a complexity-adherence trade-off: too much optimization backfires.
Willpower is finite. Behavior change research consistently shows that habit formation takes sustained effort: median time to automaticity is 59-66 days, with individual ranges from 4 to 335 days (19). During that formation period, you're drawing on limited self-regulatory resources. The more behaviors you're trying to establish simultaneously, the more you deplete those resources.
Competing demands are real. Your clients have jobs, families, responsibilities. A protocol designed for a professional athlete with 20 hours weekly to devote to health optimization isn't realistic for a busy executive or a parent of young children. The "perfect" protocol that doesn't fit their life will be abandoned.
Research on the Adherence Paradox¶
A trial in prediabetic adults tested whether augmenting or re-sequencing program components for slow responders would improve outcomes. The result? No long-term advantage from augmentation or re-sequencing, and the augmented sequence actually reduced self-efficacy (20).
Adding complexity didn't help. It may have made things worse by undermining clients' confidence.
Health coaching meta-analyses show small-to-moderate improvements in quality of life, self-efficacy, and outcomes, with effect sizes around 0.3-0.6 (21). These aren't dramatic transformations. They're sustainable, meaningful improvements built on realistic protocols.
Practical Applications¶
Start simpler than you think necessary. If your instinct is to give a client three interventions, try two. If you're tempted to add a fourth supplement, wait. Build confidence and systems before adding complexity.
Track adherence, not just outcomes. A client who "fails" at a complex protocol may succeed at a simpler one. The failure isn't the client. It's the protocol-client mismatch. Treat low adherence as a design problem you and your client can solve together, not a character flaw. Ask regularly: "What percentage of the time are you doing this?" Anything below 70-80 percent signals the need to simplify.
Celebrate sustainable wins. A client who walks 20 minutes daily for 6 months has achieved more than a client who did intense workouts for 3 weeks before burning out. Help clients see that consistency trumps intensity.
[CHONK: "Majoring in the Minor" Prevention]
"Majoring in the Minor" Prevention¶
"Majoring in the minor" is a common pattern with longevity-focused clients (and honestly, it’s an easy trap to fall into). They get really focused on marginal optimizations while their foundational behaviors are still a bit wobbly.
Recognizing the Pattern¶
The Cold Plunge Obsession
Your client has a $5,000 cold plunge in their garage, follows precise Huberman protocols (2-3 minutes at 50°F, four times weekly), and can cite the research on dopamine and norepinephrine increases.
But they’re also sleeping 5 hours a night and haven’t done strength training in years.
Cold exposure may offer benefits for resilience and metabolic health, but the effect sizes are modest, and most evidence comes from small studies. Sleep deprivation, meanwhile, is associated with 14-34 percent increased mortality risk, which makes the hierarchy pretty clear.
The Supplement Stack
Your client spends $500/month on supplements like NMN, berberine, sulforaphane, CoQ10, and a dozen others, and has researched each one carefully.
But they skip vegetables, rarely hit protein targets, and haven’t had bloodwork in three years.
Even the best supplements tend to deliver marginal effects compared to adequate nutrition. Without bloodwork, you don’t know what deficiencies (if any) actually exist, so it’s hard to match the “stack” to a real need.
The Sauna Maximizer
Your client does sauna 5 times weekly, following the Finnish studies showing cardiovascular benefits, and they’ve optimized temperature and duration.
But they also struggle to fit in two strength training sessions weekly.
Sauna is a Tier 3 intervention, while strength training is Tier 1, so the order you tackle them in matters. If you see a bit of yourself in these examples, that’s normal; many coaches do. (We get it.)
The "Basics Audit" Framework¶
If you suspect a client is majoring in the minor, the Longevity Basics Audit can help. It’s a simple checklist (included below) that helps you confirm whether Tier 1 fundamentals are in place before you spend time and energy on Tier 2-4 optimizations.
The principle: Don't optimize what isn't yet adequate.
The Longevity Basics Audit Checklist¶
This checklist helps you assess whether your client has fundamentals in place before adding optimizations. This complements the Deep Health Assessment from Chapter 1.3.
Tier 1: Non-Negotiables (Check all that apply)
Sleep
- [ ] Consistently sleeping 7-9 hours per night
- [ ] Regular sleep/wake schedule (±30 minutes)
- [ ] No undiagnosed sleep disorders
Movement
- [ ] 150+ minutes of physical activity weekly
- [ ] Includes some strength training (2+ sessions/week)
- [ ] Includes some cardiovascular training
Nutrition
- [ ] Eating adequate protein (target: 30g+ per meal)
- [ ] Regular vegetable consumption (5+ servings daily)
- [ ] Minimal ultra-processed food intake
Social Connection
- [ ] Regular meaningful contact with friends/family
- [ ] Not socially isolated
- [ ] Sense of belonging to community
Health Basics
- [ ] Annual bloodwork
- [ ] No smoking
- [ ] Alcohol within recommended limits (≤2-4 drinks/week)
Scoring
- 10-12 checked: Foundation solid. Ready for Tier 2-3 optimizations
- 6-9 checked: Foundation needs work. Prioritize unchecked items before optimizing
- 0-5 checked: Foundation critical. Focus exclusively on Tier 1 until 8+ items checked
Connection to Deep Health Assessment
You can map results to your client's Deep Health Assessment (Chapter 1.3):
- Sleep gaps → Physical and Mental dimensions
- Movement gaps → Physical and Emotional dimensions
- Nutrition gaps → Physical dimension
- Social gaps → Social/Relational and Emotional dimensions
- Health basics gaps → Physical dimension
Together, these two assessments help you identify WHERE to start with each client.
Coaching Conversations for Redirection¶
Redirecting a client away from optimization and toward foundations works best when you lead with curiosity rather than dismissal. The goal isn’t to shame their interest in biohacking; it’s to help them aim that motivation at the highest-return actions first.
Coaching in Practice: Redirecting the Biohacker¶
[CHONK: Coaching in Practice - Redirecting the Biohacker]
The scenario: A client who's deep into biohacking wants to add rapamycin to their protocol.
What NOT to do:
❌ Say "That's too advanced for you" or "You're not ready for that."
Why it doesn't work: It dismisses their effort, creates defensiveness, and it skips the most useful part, which is understanding what's driving their interest.
What TO do:
✅ Acknowledge their curiosity, get curious yourself, and then connect their question back to the hierarchy.
Sample dialogue:
Client: "I've been researching rapamycin. What do you think about adding it to my protocol?"
Coach: "You've clearly gone down the rabbit hole on this, so I'm curious: what about rapamycin is most interesting to you?" (It really is fascinating.)
Client: "Honestly, I just don't want to end up like my dad, who had heart disease in his 50s, so I want to do everything I can."
Coach: "That makes a lot of sense. Wanting to avoid what you saw in your dad is a powerful motivator, and also a lot to carry." [Pause] "Can I ask a couple of questions about the basics before we talk about rapamycin specifically?"
Client: "Sure, go ahead."
Coach: "Before we get into rapamycin, how has your sleep been this past week?"
Client: "Pretty rough. I’m getting five, maybe six hours a night because I’m up late working and then scrolling."
Coach: "Got it, and how about movement? Tell me what a typical week of exercise looks like for you."
Client: "I keep meaning to lift, but it usually doesn't happen. I sit most of the day."
Coach: "Thanks for being honest. You're definitely not alone there, and here's the interesting part: rapamycin is still being studied for longevity, and the effect sizes in humans are uncertain. Sleep and movement, on the other hand, have massive, well-established effects on every system we care about."
Client: "So you think I shouldn't take it?"
Coach: "That's a decision to make with your doctor. From a coaching perspective, I want to make sure you're getting the big wins first. What if we spent the next three months getting your sleep and movement solid and then, if you're still interested, we revisit this conversation from a much stronger foundation?" (This often makes the next steps a lot clearer.)
Key takeaway: Acknowledge their interest, share the hierarchy logic, and redirect without judgment. They’re not wrong to be curious; they’re just working out of sequence.
When Optimization Obsession Signals Something Deeper¶
Sometimes "majoring in the minor" isn't just a sequencing issue; it can also be a signal that something deeper is going on. If this feels like a heavier topic, that's because it is, and it's okay to take it seriously.
Health anxiety can drive obsessive optimization. A client who needs to control every variable may be managing anxiety about mortality, aging, or control, which is beyond coaching scope but worth recognizing (Chapter 1.5). If you suspect clinical anxiety, refer appropriately; you’re not diagnosing, just noticing patterns.
Perfectionism can show up as never-good-enough optimization, where no matter how much the client does, there’s always something else to add. In that case, the client may benefit more from exploring identity and values (covered more in Chapter 26) than from piling on additional interventions.
Avoidance can hide behind complexity, too. A client who’s focused on obscure supplements may be avoiding harder changes, like quitting alcohol or addressing relationship issues; the advanced stuff is interesting, but the basics can feel uncomfortable.
In these cases, the issue often isn’t a lack of information about the hierarchy, but the underlying psychology, which means your job is to use your coaching skills to explore what’s driving the behavior while staying in scope. And if you’re feeling uncertain, that’s actually a sign of wisdom.
[CHONK: When Knowing Isn't Enough]
When Knowing Isn't Enough: Finding the Real Barrier¶
So your client knows they need more sleep. They've heard it from their doctor, read it in articles, and maybe even tracked their sleep and seen the data. They agree it's important, but still nothing changes.
It's one of the most common situations in coaching: the client has the information and the motivation (at least they say they do), yet the behavior doesn't happen.
Before you can help them, you need to understand what's actually in the way. In our experience, it comes down to one of three things:
The Three Barriers: Skills, Motivation, Conditions¶
When a behavior isn't happening, the barrier falls into one of three categories. Once you know which one you’re dealing with, the next step gets much clearer.
1. Skills: Do they know how?
This is about capability: can they actually do the behavior, not just understand that they should?
- Do they know what to do and how to do it? (Knowledge + know-how)
- Can they physically do it? (Physical ability)
2. Motivation: Do they actually want to?
This is about drive: is the desire there in real life, not just in words?
- Do they believe this behavior will help?
- Do they genuinely want to do it, or just think they "should"?
- Do they believe they can succeed?
- What else do they want that might conflict, like downtime at night, work demands, or time with family?
Even when motivation is real, the next question is whether their current setup makes the behavior doable.
3. Conditions: Does their life allow it?
This is about environment and circumstances: even with skills and motivation, does their world support this behavior?
- Do they have the time and resources (money, equipment, access)?
- Does their physical and social environment support it?
Why This Matters¶
Different barriers require different solutions, and using the wrong solution for the barrier is like prescribing glasses for a broken leg.
| Barrier | What Works | What Doesn't Work |
|---|---|---|
| Skills | Education, training, skill-building, simplification | Motivational speeches, environmental changes alone |
| Motivation | Values work, exploring benefits, building confidence, addressing fears | More information, environmental changes alone |
| Conditions | Environmental restructuring, removing friction, providing resources | More education, trying harder |
The most common coaching mistake is assuming the barrier is always motivation: "If they wanted it enough, they'd do it." Often, that's not what's happening at all.
Coaching in Practice: Diagnosing the Real Barrier¶
What NOT to do (assume it's motivation):
Client: "I know I need more sleep, but I just can't seem to do it."
Coach: "You just have to want it more and try harder to get to bed earlier."
Client: "I do want it. I just keep getting pulled into work and then I scroll to unwind."
Coach: "Well, you have to make it a priority and stick to it."
A better approach (figure out which barrier it is):
Client: "I know I need more sleep, but I just can't seem to do it."
Coach: "You’ve done the homework, you believe it matters, and you’re still stuck. When you don’t get to bed on time, what usually gets in the way?"
Client: "Work runs late, and then my brain feels wired. I end up scrolling until I pass out."
Coach: "Got it. That sounds like a mix of conditions (work running late) and skills (a way to downshift that isn’t your phone). Want to pick one small experiment for this week, like a 10-minute wind-down that starts at a set time, even if bedtime isn’t perfect?"
Client: "Yeah, I can do 10 minutes."
Coach: "Great. We'll make it specific and easy, then we’ll see what gets in the way and adjust."
[CHONK: Coaching in Practice - Diagnosing the Real Barrier]
Client: Sarah, 47, has been trying to "eat healthier" for months. She knows what to do and she's motivated (her doctor flagged elevated blood sugar), but her eating patterns still haven't changed.
What NOT to do:
❌ Assume it's a motivation problem and give her more reasons why nutrition matters.
Why it doesn't work: She already knows it matters, and more information won't help if information isn't the barrier.
What TO do:
✅ Instead, diagnose which barrier is actually operating.
Sample dialogue:
Coach: "You mentioned you've been wanting to improve your eating but haven't made the changes you want. I'm curious: when you imagine eating the way you want to, what gets in the way?"
Sarah: "I just don't have time to cook. By the time I get home from work, I'm exhausted, and the kids need to eat now. So we order takeout or I throw together whatever's fastest."
Coach: "That makes sense. So it's less about not knowing what to eat or not wanting to eat well. It's more that your evenings don't really allow for it?"
Sarah: "Exactly. I know what I should be eating and I want to eat that way, but my life doesn't cooperate."
Coach: "Okay, so the barrier is conditions, not skills or motivation. That's actually helpful, because it means we can focus on making healthy eating easier to fit into your real life, not convince you it's important, since you already know that."
Where this leads:
Coach: "If weeknights are the pinch point, would it help if we looked at a few options and picked the easiest one to try first?"
Sarah: "Yes. I just need something realistic."
Now the coach can explore condition-focused solutions:
- Batch cook on weekends, so weeknights are mostly reheating and assembling
- Choose healthier takeout options (not all takeout is equal), and keep a short list of go-to orders
- Keep a few simple 15-minute meals on hand, with ingredients you can pull together fast
- Use grocery delivery with pre-planned healthy items, so the default choices are already in your kitchen
- Involve kids in simple meal prep, which can make weeknights easier and build a routine
Notice how different this is from lecturing Sarah about blood sugar or giving her more nutrition information. The barrier wasn't knowledge or desire; it was circumstances.
Quick Diagnostic Questions¶
When a client isn't making progress on a behavior, you can walk through these questions together.
Coach: "Before we troubleshoot, can we figure out what kind of barrier this is: skills, motivation, or conditions?"
Client: "Sure."
Skills check: To see whether this is a skills issue, you might ask:
- Coach: "Walk me through how you'd do this, step by step, and tell me what each step would be."
- Coach: "Have you done this before, and if so, what happened when you tried?"
- Coach: "What part feels unclear or confusing right now, and what would make it feel more straightforward?"
Motivation check: To check motivation, you might ask:
- Coach: "On a scale of 1-10, how important is this to you right now?"
- Coach: "What would be different in your life if this changed?"
- Coach: "What concerns do you have about making this change?"
Conditions check: To check conditions, you might ask:
- Coach: "Where would this realistically fit in your day, and what would need to shift to make that happen?"
- Coach: "What would need to be in place for this to work consistently (time, food, equipment, support)?"
- Coach: "Who or what might get in the way, especially on your busiest days?"
Client: "Okay, that helps. I can see where this is breaking down."
The answer tells you where to focus your coaching.
Connecting to the Hierarchy¶
This three-barrier model applies directly to the Hierarchy of Longevity Needs.
When a client's Longevity Basics Audit shows gaps, don't just identify what they're missing. Diagnose why it's missing.
| Audit Gap | Common Barrier | Typical Solution |
|---|---|---|
| Not sleeping 7-9 hours | Often conditions (schedule, environment, responsibilities) | Environmental restructuring, schedule problem-solving |
| No strength training | Often skills (don't know how, intimidated by gym) | Education, training, starting simple |
| Low protein intake | Could be skills (don't know protein sources) or conditions (no time to cook) | Depends on diagnosis |
| Social isolation | Often conditions (no obvious community) or motivation (anxiety, past hurt) | Depends on diagnosis |
The audit tells you WHERE to focus; the barrier diagnosis tells you HOW to help.
For DIY Learners¶
| For DIY Learners |
|---|
| Applying this to yourself: When you're not doing something you want to do, ask yourself honestly: Is this a skills problem (I don't know how), a motivation problem (I don't actually want to, or don't believe I can), or a conditions problem (my life doesn't allow it)? Be ruthlessly honest, because we often blame motivation when it's really conditions (and vice versa), and the right diagnosis points to the right fix. If it helps, try a quick self-check: You: "What am I telling myself is the problem?" You (double-checking): "Is it actually skills, motivation, or conditions?" |
[CHONK: Adapting the Approach to Each Client]
Adapting the Approach to Each Client¶
The hierarchy in this approach gives you a useful map, but clients aren’t maps. Your job is to use the hierarchy as a guide, then adapt it to the person in front of you, including their starting point, constraints, preferences, and real-life context. And yes, this takes practice.
How to Adjust Based on Client Starting Point¶
The client who already exercises consistently
If movement is already solid, you don’t need to camp out there. Instead, do a quick scan of the other Tier 1 basics, like sleep, protein, and social connection, and then start with the biggest gaps rather than defaulting to a one-size-fits-all protocol.
The excellent sleeper who doesn't move
Great, sleep is already a strong foundation, so you can build on it by linking movement to something they already care about. You don’t have to “sell fitness” to help someone get moving.
A simple prompt that often works is:
“Since you’re already protecting your sleep, would you be open to a small experiment, like a 10-minute morning walk a few days this week?”
And when you explain the “why,” keep it grounded in evidence and simple language: Research shows that morning movement can reinforce circadian rhythm, which may improve sleep quality even further.
The socially isolated client
It can be tempting to ignore this because it feels “soft,” but it matters, and social isolation has effect sizes comparable to smoking. For this client, social connection might be the main Month 1 focus, and it often helps to make it concrete by pairing connection with something they already want or need to do.
For example, you might suggest:
- Trying a group fitness class, which builds movement and social time at once
- Setting up a walk with a friend (movement + social)
- Getting involved in a community that aligns with their values
If this feels outside your usual comfort zone, you’re not alone. You can still coach it by helping them choose tiny, doable actions that fit their life.
The client with excellent fundamentals
They exist, and if a client has sleep, movement, nutrition, and social connection dialed in, you can move into Tier 2-3 sooner. These clients may truly be ready for supplement optimization, recovery protocols, and advanced testing. Use the hierarchy, and also recognize when someone is genuinely operating at a higher tier.
Using Deep Health to Identify Gaps¶
The Deep Health Assessment (Chapter 1.3) gives you a multidimensional snapshot. Pair it with the Longevity Basics Audit to identify where each client needs to start.
Example mappings:
| Deep Health Gap | Likely Longevity Priority |
|---|---|
| Physical low, others high | Focus on movement, sleep, nutrition basics |
| Emotional low | Stress management, sleep (affects emotion regulation), social connection |
| Social/Relational low | Social connection: this IS a Tier 1 priority |
| Mental/Cognitive low | Sleep (affects cognition), movement (neurogenesis), stress management |
| Environmental low | Tier 2 environmental optimization, but only after Tier 1 is solid |
| Existential low | Purpose work: this sustains long-term adherence |
"This Is a Guide, Not a Prescription"¶
In this chapter, you’ve seen models, hierarchies, and checklists. Think of them as tools, not rules.
If you’re worried about “doing it wrong” or not following the hierarchy perfectly, that’s normal. These tools are here to support your thinking, not box you in.
Longevity coaching is fundamentally client-led (Chapter 1.5). You guide, you don't prescribe. The client chooses priorities based on their values, readiness, and life context, and your job is to:
- Help them see the hierarchy so they understand what matters most right now.
- Identify their specific gaps using assessments, then translate those results into a clear starting point.
- Offer informed recommendations based on evidence, including the trade-offs in plain language.
- Let them lead by choosing the priorities that fit their values, readiness, and real-life context.
A client who insists on starting with sauna before fixing their sleep isn’t “wrong.” They’re making a choice. Your role is to help them make an informed choice by understanding the trade-offs.
For example:
What NOT to do
Coach: “Nope. Sauna is Tier 2, so you need to fix sleep first.”
A better approach
Client: “I really want to start with sauna. Can we do that?”
Coach: “We can, if that feels doable right now. Before we start, can I share one thing that will help you get more out of it?”
Client: “Sure.”
Coach: “If sleep is still shaky, it usually limits the benefits you’ll get from most Tier 2 tools, including sauna. Would you be open to choosing one small sleep action to work on alongside sauna?”
Client: “Yeah, I can do one thing.”
Coach: “Great. What’s one simple, realistic sleep action you’d be willing to try this week?”
This is coaching, not prescribing.
[CHONK: Summary]
Summary¶
Longevity coaching success depends on prioritization. The interventions that capture attention—biohacks, exotic supplements, advanced protocols—often deliver the smallest effects. The interventions that move the needle—sleep, movement, nutrition, social connection—are foundational, not optional.
Key Takeaways¶
The Hierarchy of Longevity Needs:
- Tier 1 (Foundation): ~70% of outcomes → Sleep, movement, nutrition, social connection, health basics
- Tier 2 (Significant): ~20% of outcomes → Stress management, environment, advanced nutrition
- Tier 3 (Minor): ~9% of outcomes → Supplements, recovery protocols, testing
- Tier 4 (Marginal): ~1% of outcomes → Biohacks, experimental interventions
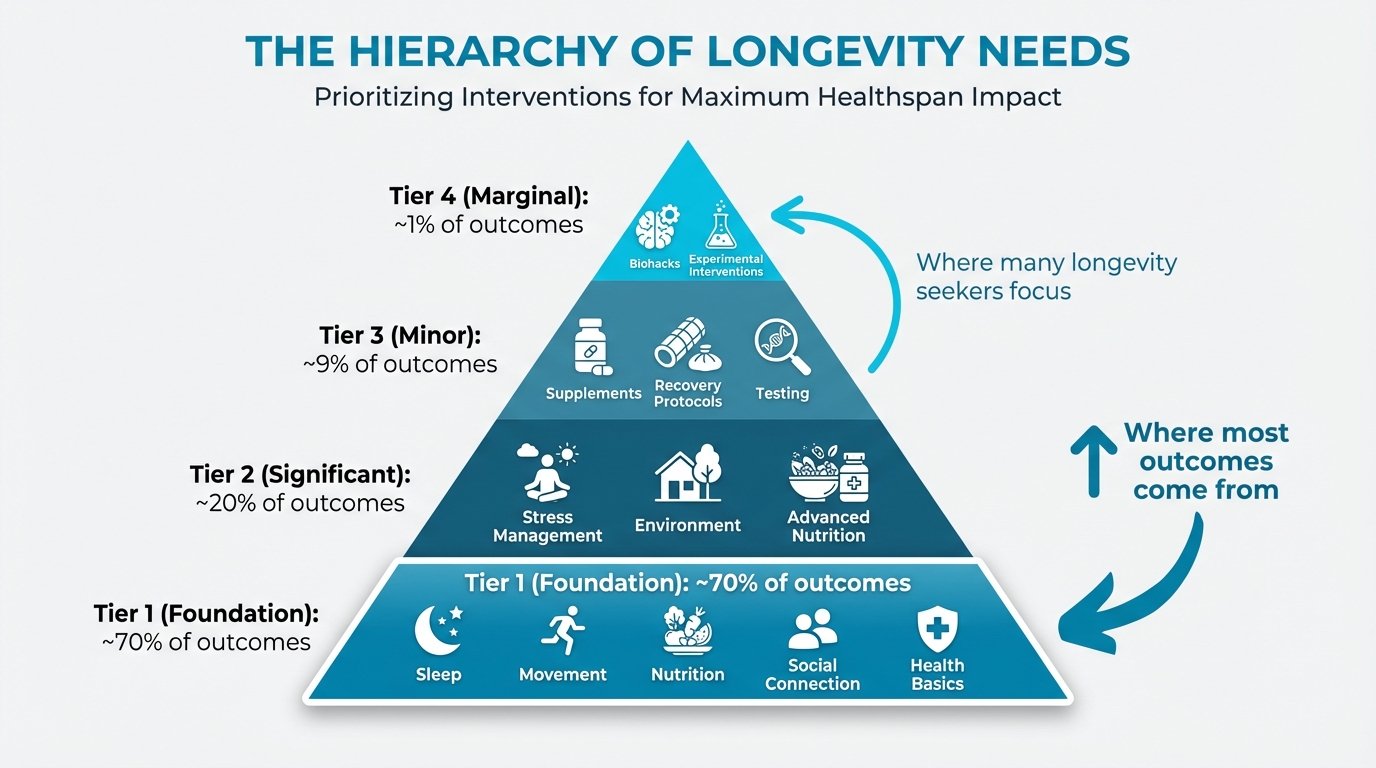
Figure: Tier 1/2/3 visual with % outcomes
The Non-Negotiables (if you do nothing else):
- 150+ minutes exercise weekly (strength + cardio), and 7-9 hours sleep consistently
- Adequate protein (30g+ per meal), plus strong social connections
- Annual bloodwork, no smoking, and limited alcohol
The Adherence Paradox:
- Aim for ~80% adherence to “good,” because that beats 40% adherence to “perfect”
- Keep protocols simple so they're sustainable; complexity often backfires
- Start with less and build gradually
The Phased Approach:
- Month 1: Foundation (1-2 core habits)
- Month 2: Expansion (add 2-3 more)
- Month 3: Optimization (fine-tune, plan long-term), adapting phases to each client's starting point
Preventing "Majoring in the Minor":
- Use the Longevity Basics Audit before adding optimizations, and don't optimize what isn't yet adequate
- When clients want to jump to “Tier 3–4” tactics, redirect with curiosity (not dismissal) and watch for deeper issues behind the obsession
Quick coaching example
What not to do:
- Coach: "Supplements are pointless. You need to sleep more."
- Client: "Okay…"
Better:
- Client: "What supplements should I take for longevity?"
- Coach: "We can talk supplements. Before we do, can I ask how sleep and workouts have been this week?"
- Client: "Honestly, not great."
- Coach: "That helps. Let's shore up Tier 1 first, then we can decide whether any Tier 3 tools are worth adding."
What's Coming Next¶
In Chapters 23-25, you'll apply this prioritization approach to detailed case studies: the stressed executive, the aging athlete, and the health-anxious optimizer. You'll see how the hierarchy translates to real coaching conversations and multi-year plans.
In Chapter 26, you'll go deeper on behavior change psychology and how to help clients shift their identity to sustain long-term change; in Chapter 27, you'll learn about creating your longevity coaching practice, including the business and professional dimensions of this work.
For now, remember the core principle: Don't biohack before you sleep. Help your clients build the foundation first, because everything else becomes more effective when the basics are in place.
[CHONK: Study Guide Questions]
Study Guide Questions¶
Use these questions to review the material and get ready for the chapter exam. They’re optional, but answering even a few can help you learn actively and quickly spot anything you might want to revisit. If you can’t answer all of them yet, that’s completely normal.
-
What are the four tiers of the Hierarchy of Longevity Needs, and approximately what percentage of outcomes does each tier contribute?
-
List the six Non-Negotiables from the longevity protocol, and note which has the strongest evidence for mortality reduction.
-
Explain the Adherence Paradox in your own words. Why does "80% adherence to good" beat "40% adherence to perfect"?
-
A client asks about starting a complex supplement stack, but they currently sleep 5-6 hours and don't exercise regularly. How would you respond using the concepts from this chapter?
-
What is "majoring in the minor" syndrome? Give two examples of how it might appear in a longevity-focused client.
-
How does the Longevity Basics Audit connect to the Deep Health Assessment from Chapter 1.3?
-
Describe how you would adapt the Month 1/2/3 phased approach for a client who already has excellent sleep habits but doesn't exercise.
-
A client scores 5/12 on the Longevity Basics Audit but wants to focus on sauna protocols and cold exposure. Using this chapter's principles, how would you approach this coaching conversation?
-
What role does social connection play in the Hierarchy of Longevity Needs, and what effect size is associated with social isolation?
-
How do you balance the structured approach of the hierarchy with the PN principle that coaching should be client-led, not prescriptive?
Optional readings¶
If you’d like to explore a bit more, these articles dig into a few key topics from this chapter in extra detail.
- Implementation Science for Longevity Coaches: The science of getting things done: why people don't do what they know they should, and how to help them close that gap, including the full model behind "skills, motivation, conditions" barrier diagnosis.
References¶
-
Lo W, Hu T, Shih C, Lin H, Hwang J. Impact of Healthy Lifestyle Factors on Life Expectancy and Lifetime Health Care Expenditure: Nationwide Cohort Study. JMIR Public Health and Surveillance. 2024;10:e57045. doi:10.2196/57045
-
Jackowska B, Wiśniewski P, Noiński T, Bandosz P. Effects of lifestyle-related risk factors on life expectancy: A comprehensive model for use in early prevention of premature mortality from noncommunicable diseases. PLOS ONE. 2024;19(3):e0298696. doi:10.1371/journal.pone.0298696
-
Todd B. How much do solutions to social problems differ in their effectiveness? 80,000 Hours; 2023. https://80000hours.org/2023/02/how-much-do-solutions-differ-in-effectiveness/
-
Martinez-Gomez D, Luo M, Huang Y, Rodríguez-Artalejo F, Ekelund U, Sotos-Prieto M, et al. Physical Activity and All-Cause Mortality by Age in 4 Multinational Megacohorts. JAMA Network Open. 2024;7(11):e2446802. doi:10.1001/jamanetworkopen.2024.46802
-
Eberth S, et al. Daily steps and all-cause mortality: An umbrella review and meta-analysis. Prev Med; 2024. https://pubmed.ncbi.nlm.nih.gov/38901742/
-
Ungvari Z, Fekete M, Varga P, Fekete JT, Lehoczki A, Buda A, et al. Imbalanced sleep increases mortality risk by 14–34%: a meta-analysis. GeroScience. 2025;47(3):4545-4566. doi:10.1007/s11357-025-01592-y
-
Wang F, Gao Y, Han Z, Yu Y, Long Z, Jiang X, et al. A systematic review and meta-analysis of 90 cohort studies of social isolation, loneliness and mortality. Nature Human Behaviour. 2023;7(8):1307-1319. doi:10.1038/s41562-023-01617-6
-
Sotos-Prieto M, Bhupathiraju SN, Mattei J, Fung TT, Li Y, Pan A, et al. Association of Changes in Diet Quality with Total and Cause-Specific Mortality. New England Journal of Medicine. 2017;377(2):143-153. doi:10.1056/nejmoa1613502
-
Laukkanen T, Khan H, Zaccardi F, Laukkanen JA. Association Between Sauna Bathing and Fatal Cardiovascular and All-Cause Mortality Events. JAMA Internal Medicine. 2015;175(4):542. doi:10.1001/jamaininternmed.2014.8187
-
Dougherty TP, Meyer JE. Comparing Lifestyle Modifications and the Magnitude of Their Associated Benefit on Cancer Mortality. Nutrients. 2023;15(9):2038. doi:10.3390/nu15092038
-
Krakauer NY, Krakauer JC. Diet Composition, Anthropometrics, and Mortality Risk. International Journal of Environmental Research and Public Health. 2022;19(19):12885. doi:10.3390/ijerph191912885
-
BMC Public Health. Living healthier for longer: Comparative effects of three heart-healthy behaviors on life expectancy with and without cardiovascular disease. BMC Public Health; 2009. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-9-487
-
Academic Medicine. Where population health misses the mark: breaking the 80/20 rule. Academic Medicine; 2015. https://pubmed.ncbi.nlm.nih.gov/25551859/
-
Todd B. How much do solutions to social problems differ in their effectiveness? A collection of all the studies we could find. 80,000 Hours; 2023. https://80000hours.org/2023/02/how-much-do-solutions-differ-in-effectiveness/
-
Schulz DN, Kremers SP, Vandelanotte C, van Adrichem MJ, Schneider F, Candel MJ, et al. Effects of a Web-Based Tailored Multiple-Lifestyle Intervention for Adults: A Two-Year Randomized Controlled Trial Comparing Sequential and Simultaneous Delivery Modes. Journal of Medical Internet Research. 2014;16(1):e26. doi:10.2196/jmir.3094
-
King AC, Castro CM, Buman MP, Hekler EB, Urizar GG, Ahn DK. Behavioral Impacts of Sequentially versus Simultaneously Delivered Dietary Plus Physical Activity Interventions: the CALM Trial. Annals of Behavioral Medicine. 2013;46(2):157-168. doi:10.1007/s12160-013-9501-y
-
World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. WHO; 2003. https://apps.who.int/iris/handle/10665/42682
-
Zhu J, Dallal DH, Gray RC, Villareale J, Ontañón S, Forman EM, et al. Personalization Paradox in Behavior Change Apps. Proceedings of the ACM on Human-Computer Interaction. 2021;5(CSCW1):1-21. doi:10.1145/3449190
-
Singh B, Murphy A, Maher C, Smith AE. Time to Form a Habit: A Systematic Review and Meta-Analysis of Health Behaviour Habit Formation and Its Determinants. Healthcare. 2024;12(23):2488. doi:10.3390/healthcare12232488
-
Miller CK, King D, Nagaraja HN, Fujita K, Cheavens JS. Does intervention sequence impact self-regulatory and behavioral outcomes in an adaptive trial among adults with prediabetes?. Health Psychology and Behavioral Medicine. 2024;12(1). doi:10.1080/21642850.2024.2385490
-
Boehmer KR, Álvarez-Villalobos NA, Barakat S, de Leon-Gutierrez H, Ruiz-Hernandez FG, Elizondo-Omaña GG, et al. The impact of health and wellness coaching on patient-important outcomes in chronic illness care: A systematic review and meta-analysis. Patient Education and Counseling. 2023;117:107975. doi:10.1016/j.pec.2023.107975